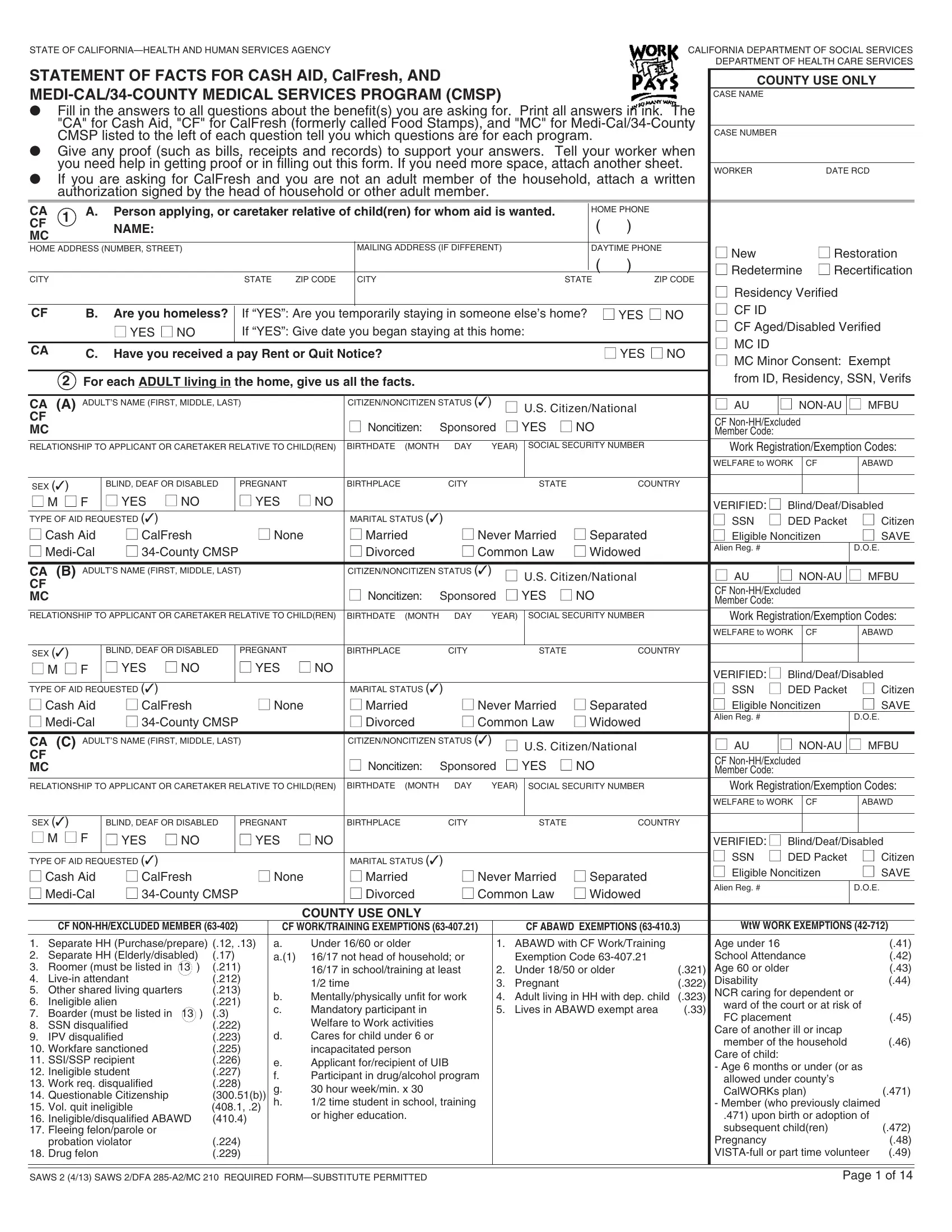
In the pursuit of assistance through social benefit programs, individuals and families navigating financial hardships in California are guided by comprehensive forms that encapsulate their current circumstances to facilitate aid provisioning. Among these, the Statement of Facts for Cash Aid, CalFresh (formerly known as Food Stamps), and Medi-Cal/34-County Medical Services Program (CMSP) stands as a pivotal document prepared by the California Department of Social Services and Department of Health Care Services. This form requires thorough information regarding the applicants' demographic, residency, and financial status, aiming to discern their eligibility and the extent of aid they require. Applicants are instructed to provide detailed responses concerning each household member's citizenship status, potential disabilities, employment, income sources, and educational pursuits while also disclosing any received or anticipated public assistance from outside California. Furthermore, it delves into specific living arrangements, such as homelessness or residing in subsidized housing, and scrutinizes the familial structure to understand the dynamics affecting dependents and childcare necessities. Emphasizing the importance of accuracy and truthfulness, the form also caters to special circumstances, including but not limited to, foster child placements, strike participations, and child or spousal support obligations. This meticulous compilation of facts not only underscores the holistic approach adopted by social services in offering support but also highlights the critical role of such documents in bridging the gap between need and aid.
| Question | Answer |
|---|---|
| Form Name | Statment Of Fact For Food Stamps Form |
| Form Length | 14 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 30 sec |
| Other names | medi, SSN, NONCITIZEN, california |
STATE OF |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
|
|
DEPARTMENT OF HEALTH CARE SERVICES |
STATEMENT OF FACTS FOR CASH AID, CalFresh, AND |
|
|
|
COUNTY USE ONLY |
|
|
CASE NAME |
|
●Fill in the answers to all questions about the benefit(s) you are asking for. Print all answers in ink. The "CA" for Cash Aid, "CF" for CalFresh (formerly called Food Stamps), and "MC" for
|
|
CMSP listed to the left of each question tell you which questions are for each program. |
|
|
|
CASE NUMBER |
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
● |
|
Give any proof (such as bills, receipts and records) to support your answers. Tell your worker when |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
you need help in getting proof or in filling out this form. If you need more space, attach another sheet. |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
WORKER |
|
|
|
|
DATE RCD |
|||||||||||||||||||||||||
● |
If you are asking for CalFresh and you are not an adult member of the household, attach a written |
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
authorization signed by the head of household or other adult member. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CA |
|
1 |
A. |
Person applying, or caretaker relative of child(ren) for whom aid is wanted. |
|
HOME PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
CF |
|
|
NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME ADDRESS (NUMBER, STREET) |
|
|
|
|
|
|
|
|
MAILING ADDRESS (IF DIFFERENT) |
|
|
|
DAYTIME PHONE |
|
|
■ New |
|
|
|
|
■ Restoration |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Redetermine |
■ Recertification |
||||||||||
CITY |
|
|
|
|
|
|
|
STATE |
|
ZIP CODE |
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Residency Verified |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ CF ID |
|
|
|
|
|
|
|
|
|
CF |
|
|
B. |
Are you homeless? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
If “YES”: Are you temporarily staying in someone else’s home? |
■ YES ■ NO |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
■ CF Aged/Disabled Verified |
|||||||||||||||||||||||||||||
|
|
|
|
■ YES ■ NO |
|
|
|
If “YES”: Give date you began staying at this home: |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
■ MC ID |
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
CA |
|
C. |
Have you received a pay Rent or Quit Notice? |
|
|
|
|
|
|
■ YES ■ NO |
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
■ MC Minor Consent: Exempt |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
2 For each ADULT living in the home, give us all the facts. |
|
|
|
|
|
|
|
|
|
|
from ID, Residency, SSN, Verifs |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
CA (A) ADULT’S NAME (FIRST, MIDDLE, LAST) |
|
|
CITIZEN/NONCITIZEN STATUS (✓) |
|
■ U.S. Citizen/National |
|
|
■ AU |
|
■ |
■ MFBU |
||||||||||||||||||||||
CF |
|
|
|
|
|
|
|
|
|
|
|
|
■ Noncitizen: |
Sponsored |
■ YES |
■ NO |
|
|
|
CF |
|
|
|
|
|||||||||
MC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Member Code: |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
RELATIONSHIP TO APPLICANT OR CARETAKER RELATIVE TO CHILD(REN) |
BIRTHDATE (MONTH |
DAY |
YEAR) |
SOCIAL SECURITY NUMBER |
|
|
|
Work Registration/Exemption Codes: |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WELFARE to WORK |
|
|
CF |
|
|
ABAWD |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEX (✓) |
|
BLIND, DEAF OR DISABLED |
PREGNANT |
|
BIRTHPLACE |
CITY |
|
|
STATE |
COUNTRY |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
■ M ■ F |
■ YES |
■ NO |
|
|
■ YES |
■ NO |
|
|
|
|
|
|
|
|
|
|
|
VERIFIED: ■ Blind/Deaf/Disabled |
|||||||||||||||
TYPE OF AID REQUESTED (✓) |
|
|
|
|
|
|
|
|
MARITAL STATUS (✓) |
|
|
|
|
|
|
|
|
■ SSN |
■ DED Packet |
|
|
■ Citizen |
|||||||||||
■ Cash Aid |
■ CalFresh |
|
|
|
■ None |
■ Married |
■ Never Married |
■ Separated |
|
|
■ Eligible Noncitizen |
|
|
■ SAVE |
|||||||||||||||||||
■ |
■ |
|
|
|
|
■ Divorced |
■ Common Law |
■ Widowed |
|
|
Alien Reg. # |
|
|
|
|
|
D.O.E. |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
CA (B) ADULT’S NAME (FIRST, MIDDLE, LAST) |
|
|
CITIZEN/NONCITIZEN STATUS (✓) |
|
■ U.S. Citizen/National |
|
|
■ AU |
|
■ |
■ MFBU |
||||||||||||||||||||||
CF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
■ Noncitizen: |
|
|
■ YES |
■ NO |
|
|
|
CF |
|
|
|
|
|||||||||
MC |
|
|
|
|
|
|
|
|
|
|
|
Sponsored |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Member Code: |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work Registration/Exemption Codes: |
||||||||
RELATIONSHIP TO APPLICANT OR CARETAKER RELATIVE TO CHILD(REN) |
BIRTHDATE (MONTH |
DAY |
YEAR) |
SOCIAL SECURITY NUMBER |
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WELFARE to WORK |
|
|
CF |
|
|
ABAWD |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEX (✓) |
|
BLIND, DEAF OR DISABLED |
PREGNANT |
|
BIRTHPLACE |
CITY |
|
|
STATE |
COUNTRY |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
■ M ■ F |
■ YES |
■ NO |
|
|
■ YES |
■ NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
VERIFIED: ■ Blind/Deaf/Disabled |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
TYPE OF AID REQUESTED (✓) |
|
|
|
|
|
|
|
|
MARITAL STATUS (✓) |
|
|
|
|
|
|
|
|
■ SSN |
■ DED Packet |
|
|
■ Citizen |
|||||||||||
■ Cash Aid |
■ CalFresh |
|
|
|
■ None |
■ Married |
■ Never Married |
■ Separated |
|
|
■ Eligible Noncitizen |
|
|
■ SAVE |
|||||||||||||||||||
■ |
■ |
|
|
|
|
■ Divorced |
■ Common Law |
■ Widowed |
|
|
Alien Reg. # |
|
|
|
|
|
D.O.E. |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
CA (C) ADULT’S NAME (FIRST, MIDDLE, LAST) |
|
|
CITIZEN/NONCITIZEN STATUS (✓) |
|
■ U.S. Citizen/National |
|
|
■ |
AU |
|
■ |
■ |
MFBU |
||||||||||||||||||||
CF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
■ Noncitizen: |
Sponsored |
■ YES |
■ NO |
|
|
|
CF |
|
|
|
|
||||||||||
MC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Member Code: |
|
|
|
|
|
|
|||||||||||||
RELATIONSHIP TO APPLICANT OR CARETAKER RELATIVE TO CHILD(REN) |
BIRTHDATE (MONTH |
DAY |
YEAR) |
SOCIAL SECURITY NUMBER |
|
|
|
Work Registration/Exemption Codes: |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WELFARE to WORK |
|
|
CF |
|
|
ABAWD |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEX (✓) |
|
BLIND, DEAF OR DISABLED |
PREGNANT |
|
BIRTHPLACE |
CITY |
|
|
STATE |
COUNTRY |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
■ M ■ F |
■ YES |
■ NO |
|
|
■ YES |
■ NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
VERIFIED: ■ Blind/Deaf/Disabled |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ SSN |
■ DED Packet |
|
|
■ Citizen |
|||||
TYPE OF AID REQUESTED (✓) |
|
|
|
|
|
|
|
|
MARITAL STATUS (✓) |
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Eligible Noncitizen |
|
|
■ SAVE |
||||||||||||||
■ Cash Aid |
■ CalFresh |
|
|
|
■ None |
■ Married |
■ Never Married |
■ Separated |
|
|
|
|
|||||||||||||||||||||
■ |
■ |
|
|
|
|
■ Divorced |
■ Common Law |
■ Widowed |
|
|
Alien Reg. # |
|
|
|
|
|
D.O.E. |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COUNTY USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
CF |
|
|
CF WORK/TRAINING EXEMPTIONS |
|
|
CF ABAWD EXEMPTIONS |
|
|
WtW WORK EXEMPTIONS |
||||||||||||||||||||||
1. |
Separate HH (Purchase/prepare) (.12, .13) |
|
a. |
Under 16/60 or older |
|
1. |
ABAWD with CF Work/Training |
|
|
Age under 16 |
|
|
|
|
|
(.41) |
|||||||||||||||||
2. |
Separate HH (Elderly/disabled) |
(.17) |
|
|
a.(1) 16/17 not head of household; or |
|
Exemption Code |
|
|
School Attendance |
|
|
|
(.42) |
|||||||||||||||||||
3. |
Roomer (must be listed in 13 |
) |
(.211) |
|
|
16/17 in school/training at least |
2. |
Under 18/50 or older |
(.321) |
|
Age 60 or older |
|
|
|
|
|
(.43) |
||||||||||||||||
4. |
|
|
(.212) |
|
|
1/2 time |
|
3. |
Pregnant |
|
|
|
(.322) |
|
Disability |
|
|
|
|
|
|
|
(.44) |
||||||||||
5. |
Other shared living quarters |
|
(.213) |
|
|
|
|
|
|
|
NCR caring for dependent or |
|
|||||||||||||||||||||
|
|
b. |
Mentally/physically unfit for work |
4. |
Adult living in HH with dep. child |
(.323) |
|
|
|||||||||||||||||||||||||
6. |
Ineligible alien |
|
|
(.221) |
|
|
ward of the court or at risk of |
|
|||||||||||||||||||||||||
|
|
|
c. |
Mandatory participant in |
|
5. |
Lives in ABAWD exempt area |
(.33) |
|
|
|||||||||||||||||||||||
7. |
Boarder (must be listed in 13 |
) |
(.3) |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
FC placement |
|
|
|
|
|
(.45) |
||||||||||||||||||||||
|
|
|
|
Welfare to Work activities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
8. |
SSN disqualified |
|
|
(.222) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Care of another ill or incap |
|
|
|
|||||||||||||||||
9. |
IPV disqualified |
|
|
(.223) |
|
d. |
Cares for child under 6 or |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
member of the household |
|
|
(.46) |
||||||||||||||||||
10. Workfare sanctioned |
|
|
(.225) |
|
|
incapacitated person |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Care of child: |
|
|
|
|
|
|
||||||||||||||
11. SSI/SSP recipient |
|
|
(.226) |
|
e. |
Applicant for/recipient of UIB |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
- Age 6 months or under (or as |
||||||||||||||||||||||
12. Ineligible student |
|
|
(.227) |
|
f. |
Participant in drug/alcohol program |
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
allowed under county’s |
|
|
|
|||||||||||||||||||
13. Work req. disqualified |
|
|
(.228) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
g. |
30 hour week/min. x 30 |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
CalWORKs plan) |
|
|
(.471) |
||||||||||||||||||
14. Questionable Citizenship |
|
(300.51(b)) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
h. |
1/2 time student in school, training |
|
|
|
|
|
|
|
|
- Member (who previously claimed |
|||||||||||||||||||||
15. Vol. quit ineligible |
|
|
(408.1, .2) |
|
|
or higher education. |
|
|
|
|
|
|
|
|
|
.471) upon birth or adoption of |
|||||||||||||||||
16. Ineligible/disqualified ABAWD |
|
(410.4) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
subsequent child(ren) |
|
|
(.472) |
|||||||||||||||
17. Fleeing felon/parole or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
probation violator |
|
|
(.224) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pregnancy |
|
|
|
|
|
|
|
(.48) |
||||||
18. Drug felon |
|
|
|
(.229) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SAWS 2 (4/13) SAWS 2/DFA
Page 1 of 14