
You can fill out the Apply For Food Stamps In Missouri form online using FormsPal's free PDF editing tool. Follow these steps to complete and save your Missouri SNAP application:
Step 1: Click the "Get Form" button at the top of this page to open the PDF in our editor.
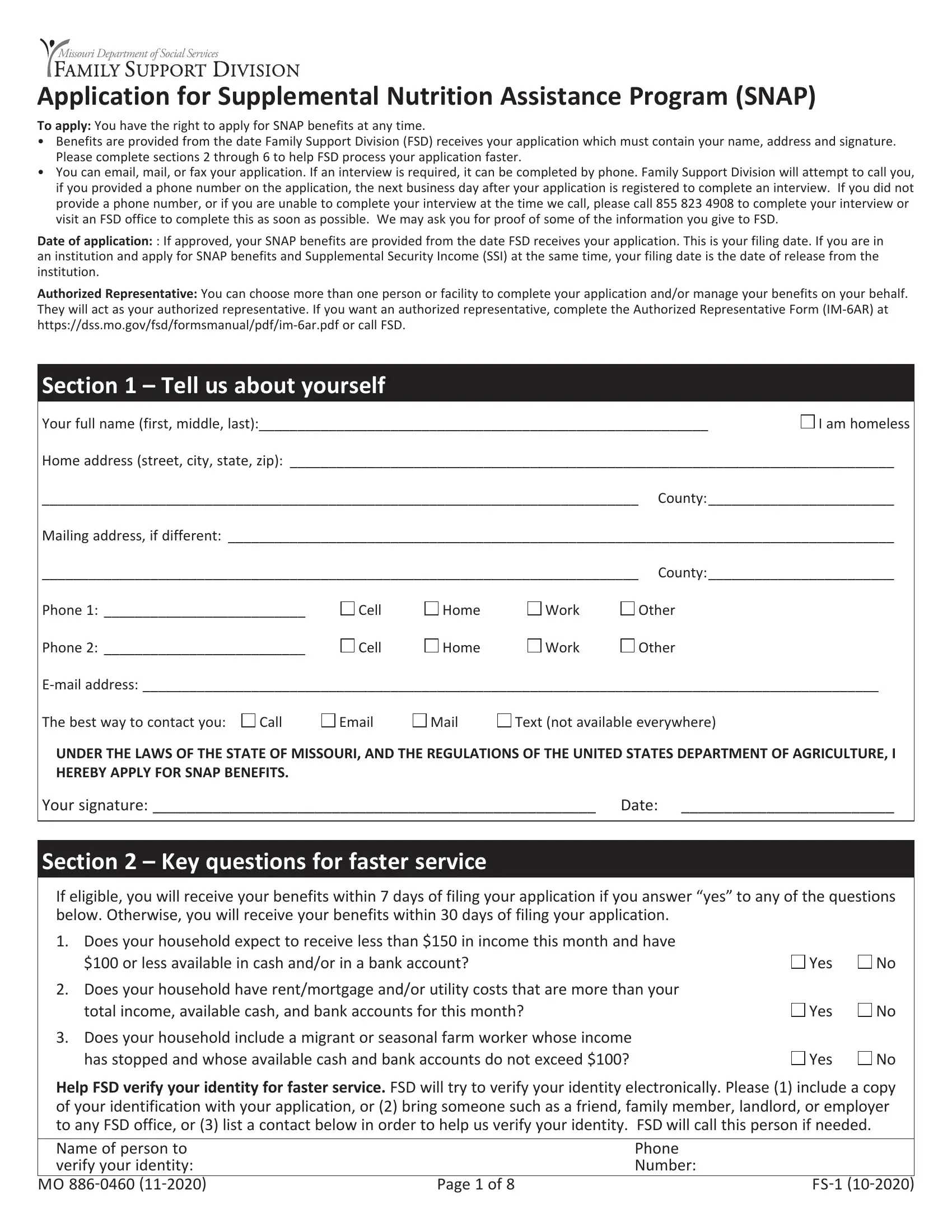
Step 2: Use the editor tools to fill in the blank fields. You can add text, upload images, and sign the document directly in your browser.
Step 3: Complete the household member section. Fill in the Full Legal Name, Sex, Relationship to Applicant, Date of Birth, SSN, and Race fields for every person in your household.
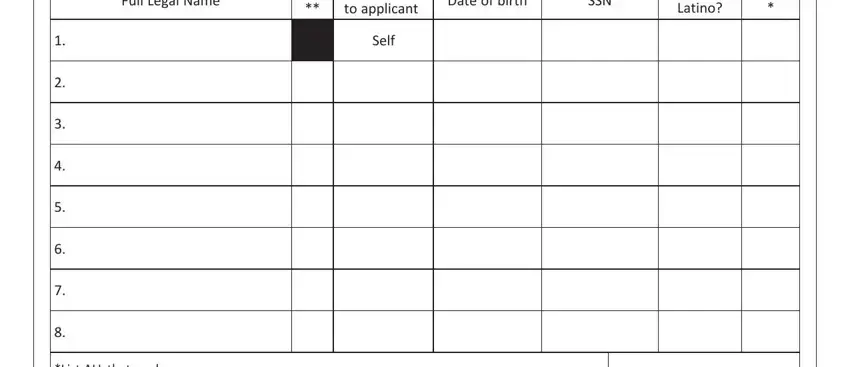
Review the Relationship to Applicant field for each household member before continuing.
Step 4: Answer questions about your household living situation. Include information about boarders, foster children, and any household members who are not U.S. citizens.
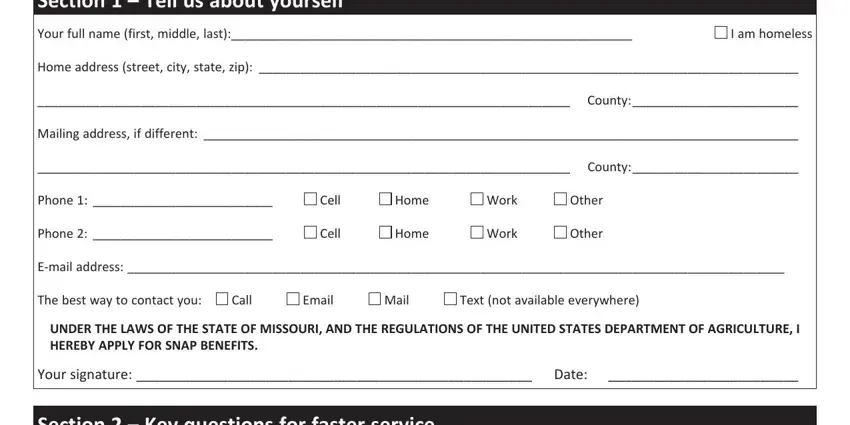
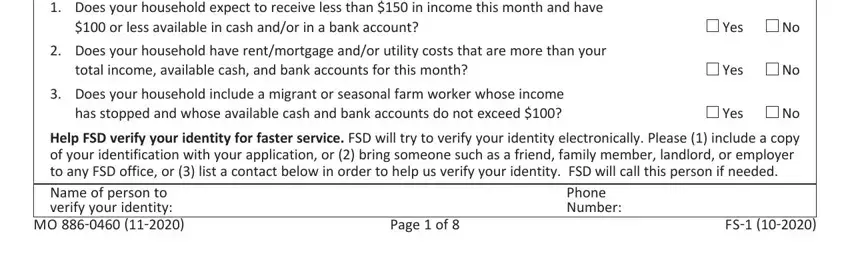
Step 5: Complete the eligibility questions. Answer yes or no to questions about prior SNAP benefits, felony convictions, and whether any household members have received duplicate benefits.
Step 6: Review your completed form, then click "Done" to save it. Your progress is automatically saved. You can return to edit the document at any time. FormsPal uses a secure system and never stores or shares your personal information.
How to Submit Your Missouri SNAP Application
Once you have filled out the form, you have several options for submitting it to the Missouri Family Support Division:
- Email: Scan your completed form and email it to your local Family Support Division office
- Mail: Print the form and mail it to your nearest Missouri DSS office
- Fax: Fax the completed application to the Family Support Division directly
- In person: Deliver the form to your local Family Support Division office during business hours
After you submit, a caseworker will contact you to schedule a phone or in-person interview. Most households receive a decision within 30 days. If approved, benefits begin from the date the application was received.
Related Missouri Assistance Forms
You may need additional forms during the SNAP application or renewal process:
- Statement of Fact for Food Stamps - used to verify household income or circumstances
- SNAP Form H1801 - used in some SNAP recertification cases
- Financial Assistance Application - for other Missouri state assistance programs