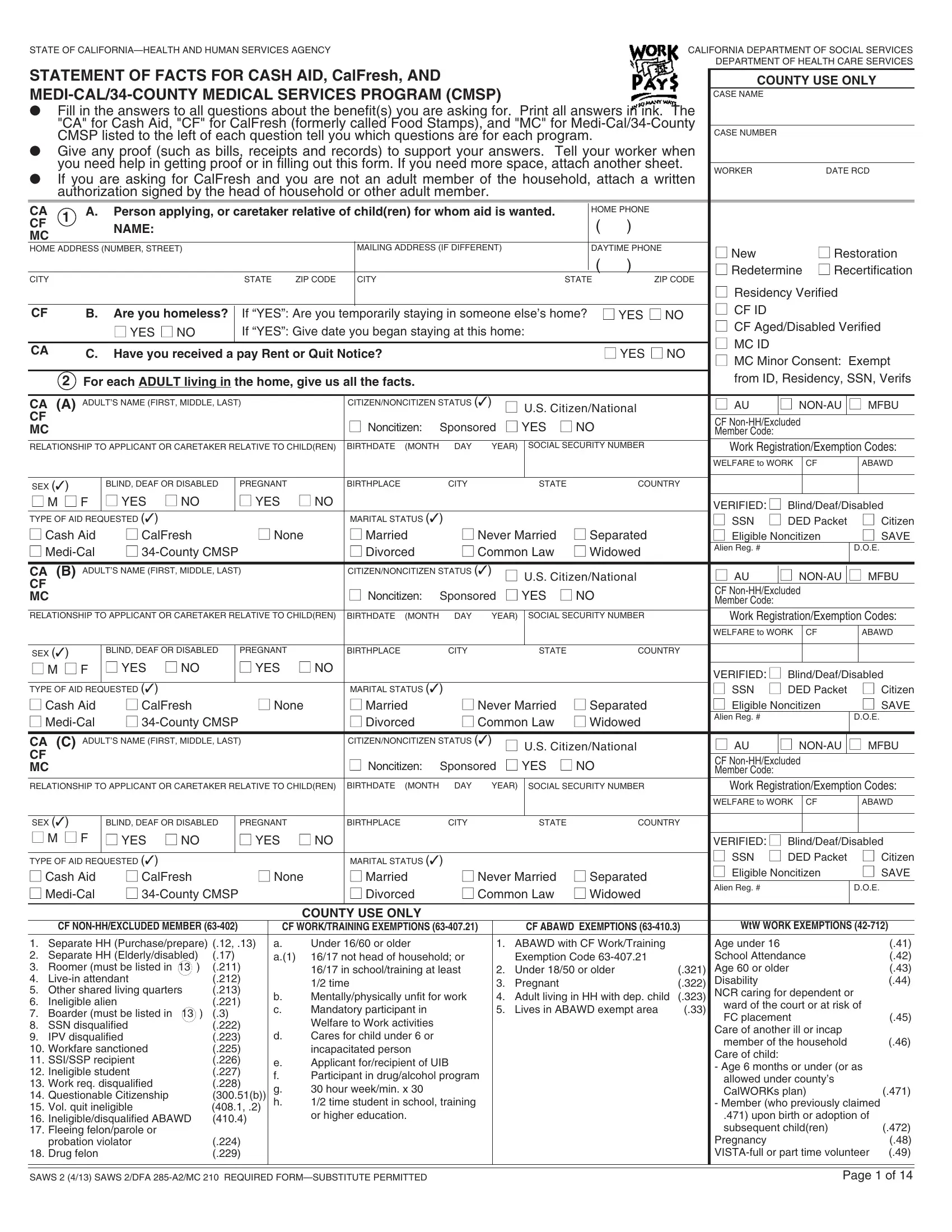
In the pursuit of assistance through social benefit programs, individuals and families navigating financial hardships in California are guided by comprehensive forms that encapsulate their current circumstances to facilitate aid provisioning. Among these, the Statement of Facts for Cash Aid, CalFresh (formerly known as Food Stamps), and Medi-Cal/34-County Medical Services Program (CMSP) stands as a pivotal document prepared by the California Department of Social Services and Department of Health Care Services. This form requires thorough information regarding the applicants' demographic, residency, and financial status, aiming to discern their eligibility and the extent of aid they require. Applicants are instructed to provide detailed responses concerning each household member's citizenship status, potential disabilities, employment, income sources, and educational pursuits while also disclosing any received or anticipated public assistance from outside California. Furthermore, it delves into specific living arrangements, such as homelessness or residing in subsidized housing, and scrutinizes the familial structure to understand the dynamics affecting dependents and childcare necessities. Emphasizing the importance of accuracy and truthfulness, the form also caters to special circumstances, including but not limited to, foster child placements, strike participations, and child or spousal support obligations. This meticulous compilation of facts not only underscores the holistic approach adopted by social services in offering support but also highlights the critical role of such documents in bridging the gap between need and aid.
| Question | Answer |
|---|---|
| Form Name | Statment Of Fact For Food Stamps Form |
| Form Length | 14 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 30 sec |
| Other names | medi, SSN, NONCITIZEN, california |
