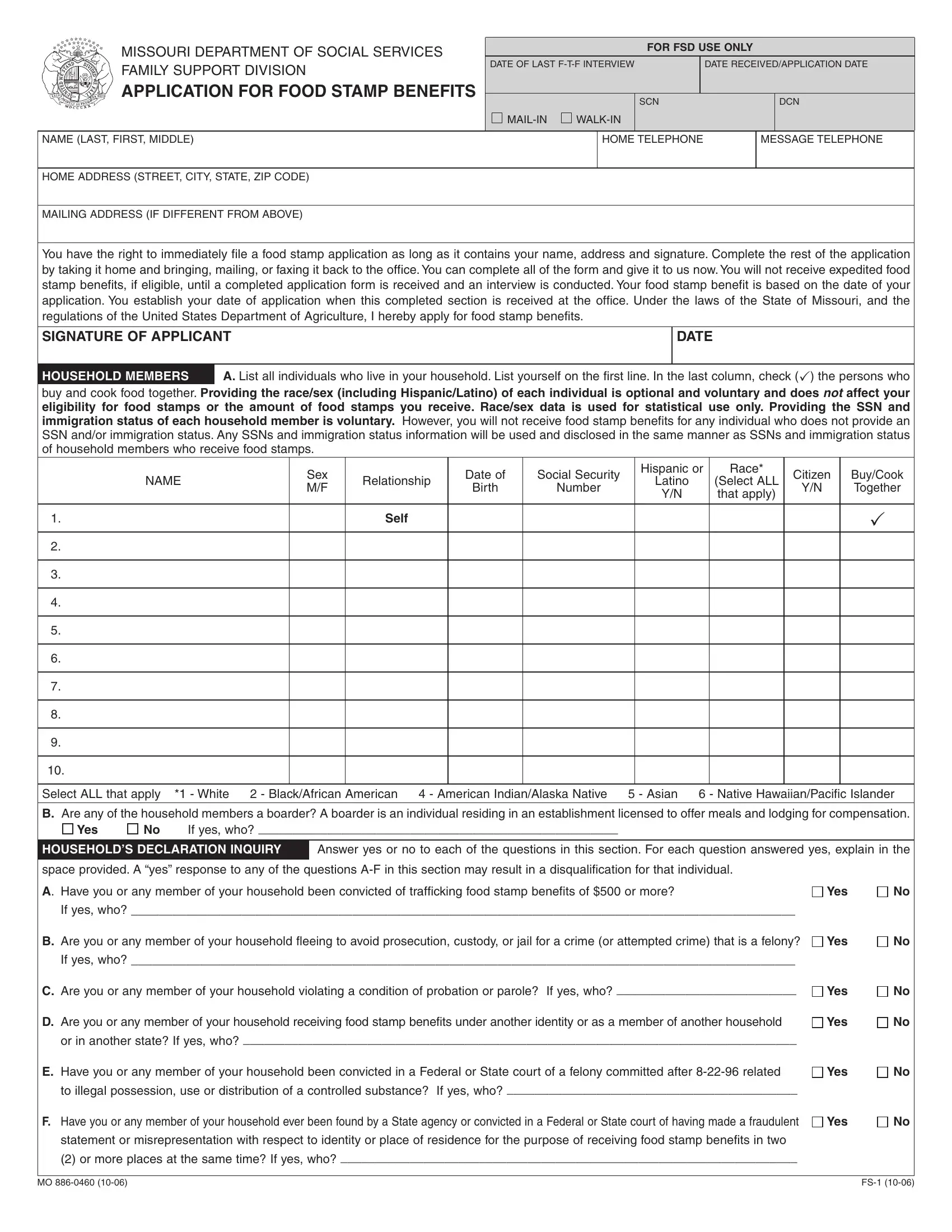
The Food Stamps Missouri form, issued by the Missouri Department of Social Services Family Support Division, is a comprehensive document that seeks to assist individuals and families in applying for food stamp benefits. This form compels applicants to provide detailed information about their household members, including name, relationship, Social Security numbers, and specifics pertaining to nationality and ethnic background. A crucial aspect of this form is its emphasis on rights and responsibilities, reminding applicants of the immediate eligibility to file as long as a name, address, and signature are provided, though a complete application and subsequent interview are necessary for the expedited processing of benefits. It highlights the eligibility criteria based on household income and expenses, underscoring the intent for quick aid provision under certain conditions. Furthermore, the document deals with serious issues like potential disqualifications arising from criminal activities related to food stamp benefits and the grave consequences of fraud, including fines and imprisonment. It also outlines the non-discrimination policy as per Federal law and the applicant's right to a fair hearing in case of benefit denial. The form is both a procedural guide and a stern warning against the misuse of the program, encapsulating the balance between offering assistance and maintaining the integrity of food stamp benefits.
| Question | Answer |
|---|---|
| Form Name | Food Stamps Missouri Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | apply for food stamps online mo, food stamps application mo, download food stamp application, missouri online food stamp application |
