
Handling PDF documents online is always very easy with our PDF editor. You can fill out std 634 timesheet here within minutes. To retain our tool on the forefront of efficiency, we strive to integrate user-oriented capabilities and improvements on a regular basis. We're always thankful for any feedback - help us with revampimg how you work with PDF forms. It just takes a few basic steps:
Step 1: First of all, open the editor by clicking the "Get Form Button" above on this page.
Step 2: With this handy PDF editing tool, you can accomplish more than merely fill out forms. Edit away and make your documents appear professional with customized textual content put in, or tweak the original input to perfection - all comes along with the capability to incorporate your personal images and sign the PDF off.
This form will require specific information; to guarantee correctness, please be sure to take heed of the following suggestions:
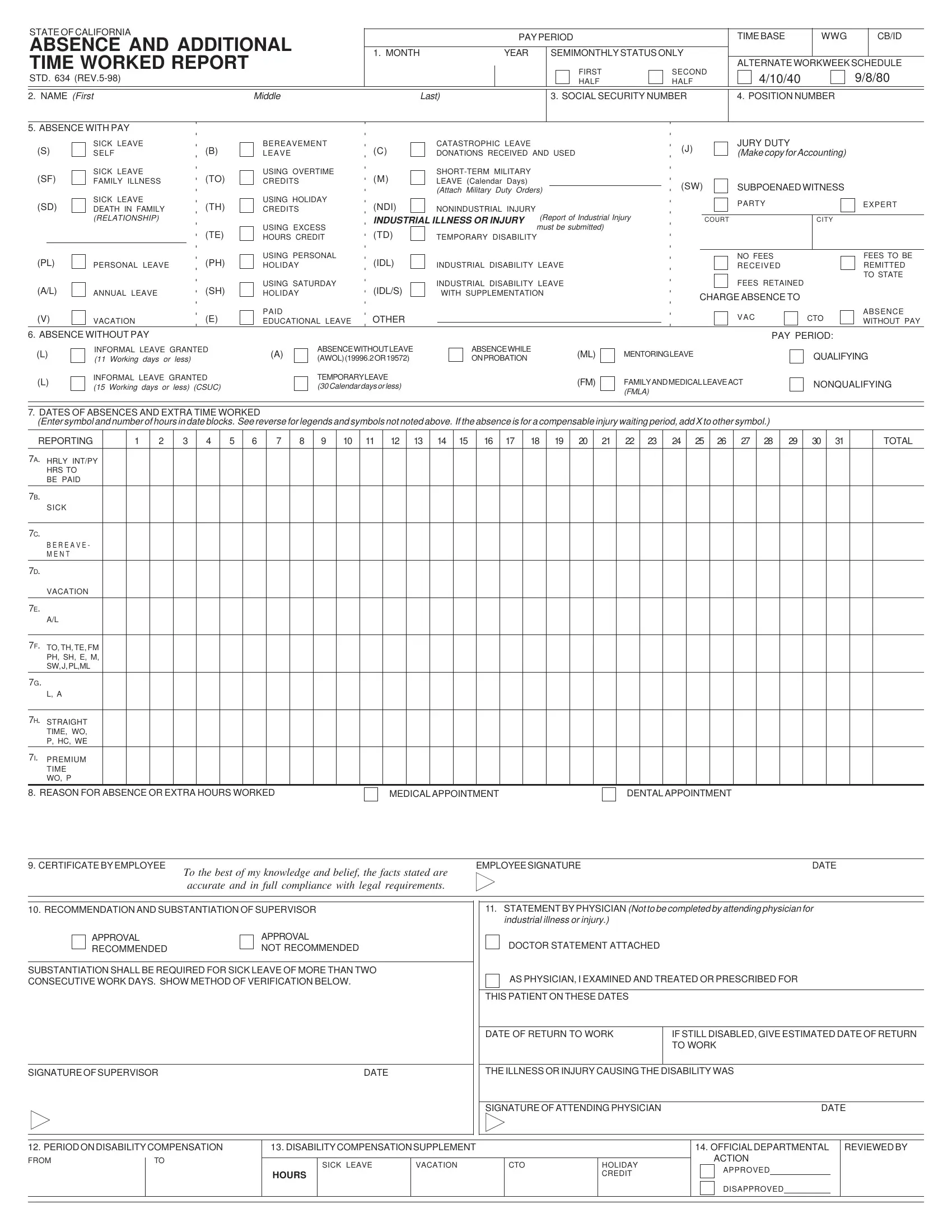
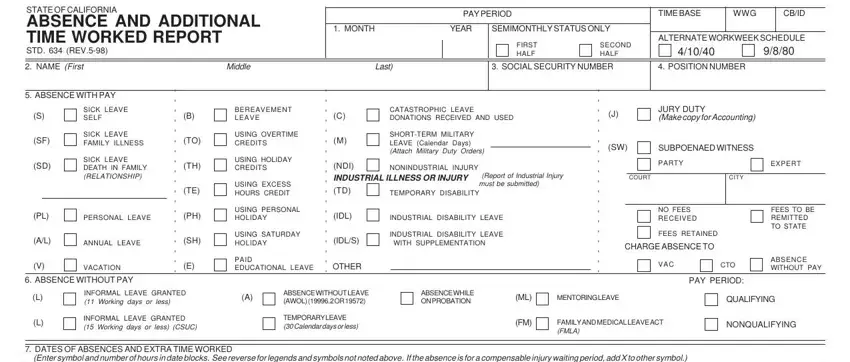
1. The std 634 timesheet requires particular information to be entered. Be sure that the next blank fields are completed:
2. Soon after the previous part is done, go to enter the applicable details in all these: REPORTING, TOTAL, HRLY INTPY HRS TO BE PAID, SICK, B E R E A V E M E N T, VACATION, TO TH TE FM PH SH E M SW J PLML, L A, STRAIGHT TIME WO P HC WE, PREMIUM TIME WO P, REASON FOR ABSENCE OR EXTRA HOURS, MEDICAL APPOINTMENT, DENTAL APPOINTMENT, CERTIFICATE BY EMPLOYEE, and To the best of my knowledge and.
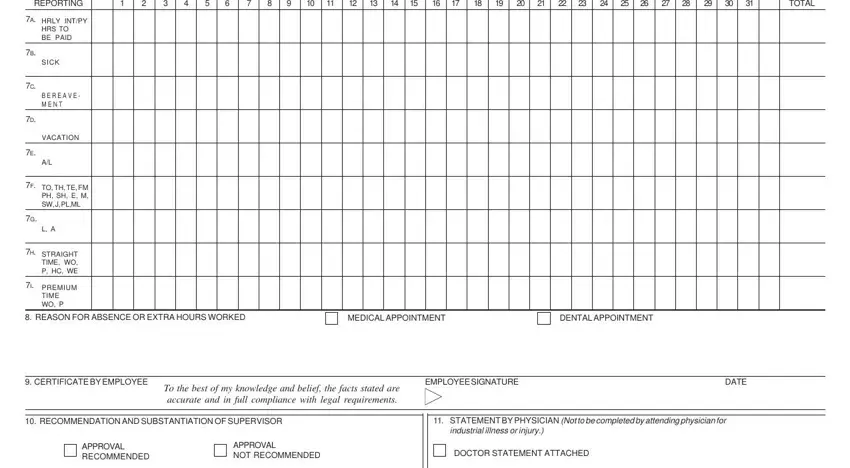
Lots of people generally make some errors while filling in VACATION in this section. Don't forget to re-examine whatever you enter here.
3. Completing SUBSTANTIATION SHALL BE REQUIRED, AS PHYSICIAN I EXAMINED AND, THIS PATIENT ON THESE DATES, SIGNATURE OF SUPERVISOR, DATE, THE ILLNESS OR INJURY CAUSING THE, DATE OF RETURN TO WORK, IF STILL DISABLED GIVE ESTIMATED, SIGNATURE OF ATTENDING PHYSICIAN, DATE, PERIOD ON DISABILITY COMPENSATION, DISABILITY COMPENSATION SUPPLEMENT, OFFICIAL DEPARTMENTAL, REVIEWED BY, and FROM is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Before finishing your form, make sure that all blanks are filled in correctly. As soon as you think it's all fine, click “Done." Right after starting a7-day free trial account here, it will be possible to download std 634 timesheet or email it right away. The form will also be at your disposal through your personal cabinet with your each edit. When using FormsPal, you'll be able to fill out forms without being concerned about data leaks or records being shared. Our secure system helps to ensure that your private details are stored safe.