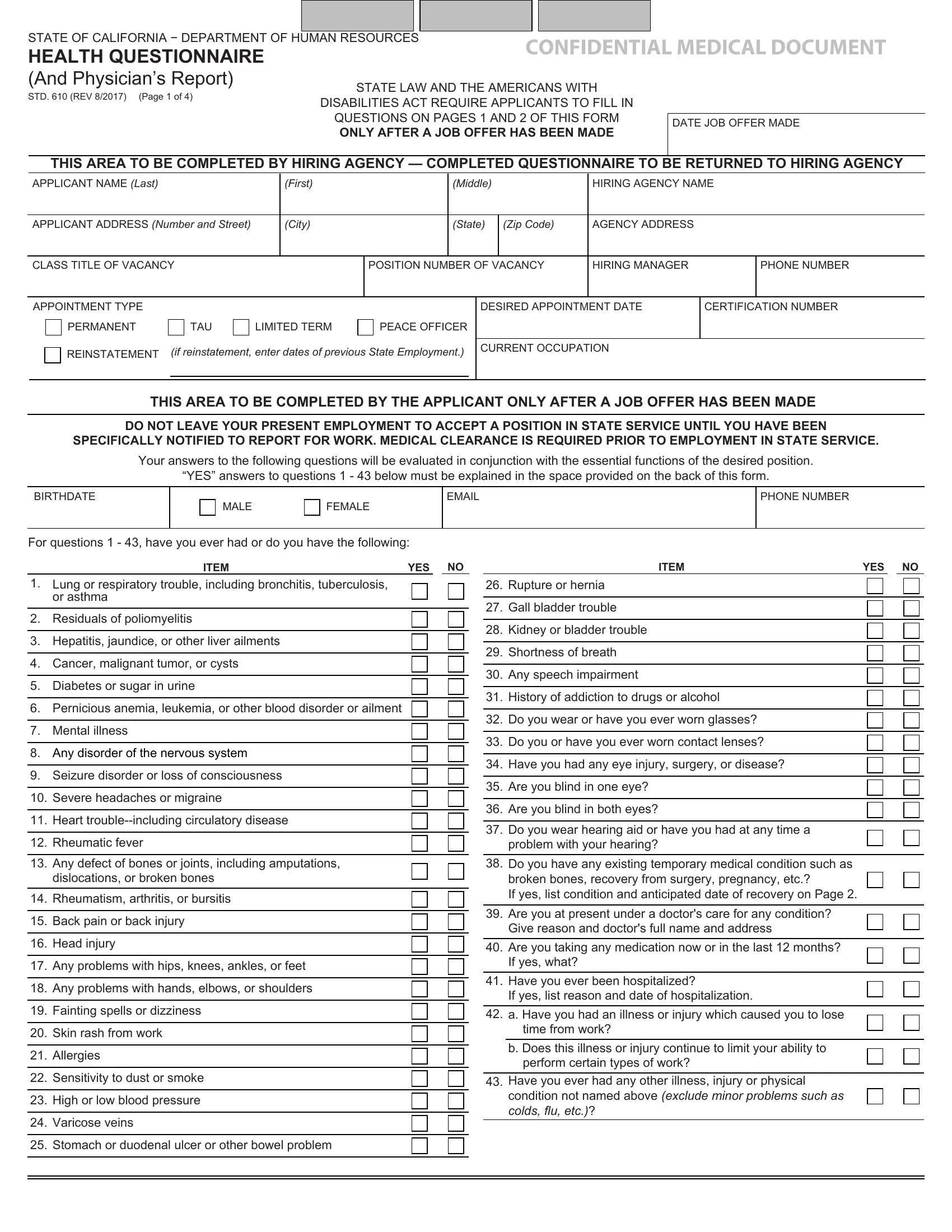
Navigating the labyrinth of employment prerequisites can often lead to encountering various forms and requirements, especially for those seeking positions within state service. Among these, the State of California - Department of Human Resources Confidential Medical Document, known as the Std 610 form, serves as a critical piece in ensuring the suitability of candidates for their roles, in alignment with state law and the Americans with Disabilities Act. This four-page document is intricately designed to collect comprehensive health-related information from applicants only after a job offer has been extended, emphasizing the state’s commitment to consider health conditions in relation to job responsibilities without breaching privacy or discrimination guidelines. The first half of the form demands candid responses from the applicant regarding a vast array of health questions, while the latter half is reserved for a detailed physician’s report. This not only facilitates a well-rounded evaluation of an applicant's medical fitness but also underlines the importance of safety and accommodation in the workplace. Through sections that require disclosure of conditions that could potentially affect job performance, to the physician’s objective remarks and a review by the California Department of Human Resources' medical officer, the Std 610 form embodies the procedural integrity and attentiveness required in the state’s hiring process. It ensures that the hiring agencies are well-informed of the medical readiness of their prospective employees, underscoring a proactive approach to workplace health and safety management.
| Question | Answer |
|---|---|
| Form Name | Std 610 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | std610, how to get form std610 completed, std 610 form, ca questionnaire template |