The Subjective Global Assessment (SGA) form serves as a fundamental tool in evaluating a patient's nutritional status, providing a comprehensive overview based on various parameters such as weight history, dietary intake, gastrointestinal symptoms, functional capacity, diagnosis or comorbidities related to nutritional needs, and physical examination. This assessment method delves into the patient's baseline and current weight to pinpoint actual weight loss over the past six months, alongside examining changes in dietary intake that might reflect a shift towards suboptimal nutrition. Gastrointestinal symptoms are meticulously recorded, offering insights into the frequency and impact of issues such as anorexia, nausea, vomiting, and diarrhea. Functional capacity is scrutinized, observing any difficulties in ambulation or activity that could signify diminished well-being. The form also accounts for the patient's primary diagnosis and any comorbidities that could alter nutritional requirements, adjusting for factors such as acute metabolic stress. A physical exam further aids in identifying signs of malnourishment, including loss of subcutaneous fat, muscle wasting, and edema. Each section contributes to an overall rating, grading the patient's nutritional status from well-nourished to severely malnourished. This intricate assessment, reviewed and updated as necessary, underscores the importance of tailoring nutritional interventions to foster patient health and recovery.
| Question | Answer |
|---|---|
| Form Name | Subjective Global Assessment Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 71 |
| Avg. time to fill out | 14 min 42 sec |
| Other names | 1-2Severely, form sga, sga form, 3-4-5Mild |
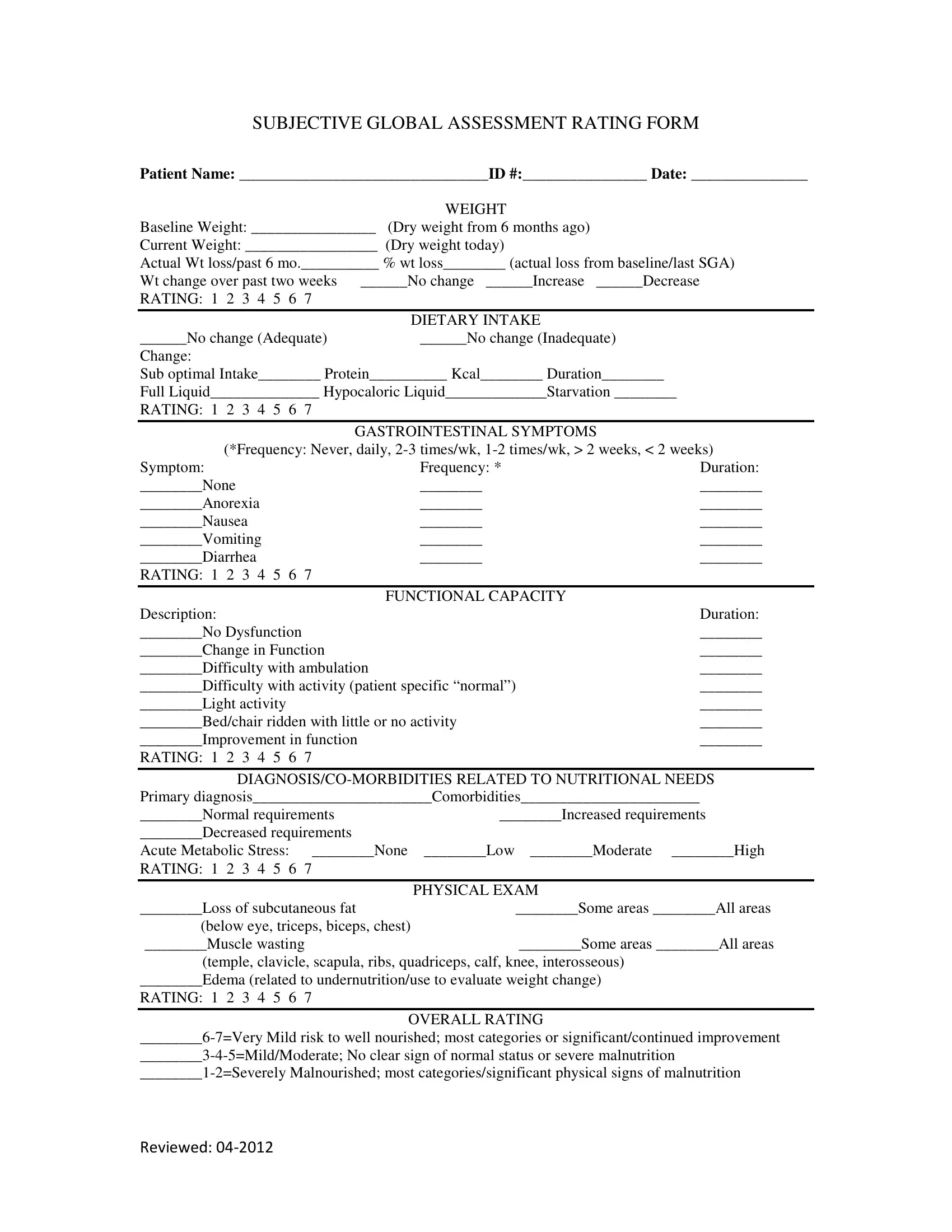
SUBJECTIVE GLOBAL ASSESSMENT RATING FORM
PATIENT NAME: ________________________________ID #:________________ DATE: _______________
WEIGHT
Baseline Weight: ________________ (Dry weight from 6 months ago)
Current Weight: _________________ (Dry weight today)
Actual Wt loss/past 6 mo.__________ % wt loss________ (actual loss from baseline/last SGA)
Wt change over past two weeks |
______No change ______Increase ______Decrease |
RATING: 1 2 3 4 5 6 7 |
|
|
|
|
DIETARY INTAKE |
______No change (Adequate) |
______No change (Inadequate) |
Change: |
|
Sub optimal Intake________ Protein__________ Kcal________ Duration________
Full Liquid______________ Hypocaloric Liquid_____________Starvation ________
RATING: 1 2 3 4 5 6 7
GASTROINTESTINAL SYMPTOMS
(*Frequency: Never, daily,
Symptom: |
Frequency: * |
Duration: |
________None |
________ |
________ |
________Anorexia |
________ |
________ |
________Nausea |
________ |
________ |
________Vomiting |
________ |
________ |
________Diarrhea |
________ |
________ |
RATING: 1 2 3 4 5 6 7 |
|
|
|
FUNCTIONAL CAPACITY |
|
Description: |
|
Duration: |
________No Dysfunction |
|
________ |
________Change in Function |
|
________ |
________Difficulty with ambulation |
|
________ |
________Difficulty with activity (patient specific “normal”) |
________ |
|
________Light activity |
|
________ |
________Bed/chair ridden with little or no activity |
________ |
|
________Improvement in function |
|
________ |
RATING: 1 2 3 4 5 6 7 |
|
|
|
|
|
________Normal requirements |
________Increased requirements |
________Decreased requirements |
|
Acute Metabolic Stress: ________None |
________Low ________Moderate ________High |
RATING: 1 2 3 4 5 6 7 |
|
|
PHYSICAL EXAM |
________Loss of subcutaneous fat |
________Some areas ________All areas |
(below eye, triceps, biceps, chest) |
|
________Muscle wasting |
________Some areas ________All areas |
(temple, clavicle, scapula, ribs, quadriceps, calf, knee, interosseous)
________Edema (related to undernutrition/use to evaluate weight change)
RATING: 1 2 3 4 5 6 7
OVERALL RATING
Reviewed:
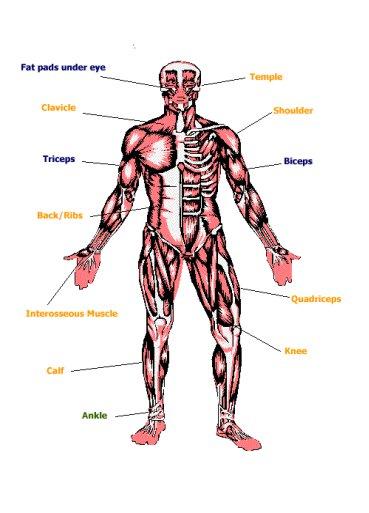
FAT AND MUSCLE STORE ASSESSMENT
Muscle (orange) stores Fat (blue) stores
Edema (green) should be assessed at the ankle. In
Date: ________________________________________________________
Patient Name: _________________________________________________
SGA Score: ___________________________________________________
Notes/Comments: ______________________________________________
Reviewed: