
If you need to fill out florida physician assistant supervision form, you won't have to install any kind of software - just make use of our online PDF editor. The tool is constantly maintained by our team, acquiring cool features and turning out to be more convenient. Getting underway is simple! All you have to do is take the next simple steps directly below:
Step 1: Firstly, access the tool by clicking the "Get Form Button" at the top of this webpage.
Step 2: With the help of our state-of-the-art PDF file editor, you can actually do more than just fill in blank form fields. Try all the functions and make your documents seem high-quality with custom text incorporated, or adjust the file's original input to perfection - all that comes along with an ability to incorporate your personal pictures and sign it off.
This form will require particular info to be filled out, so ensure you take the time to fill in exactly what is asked:
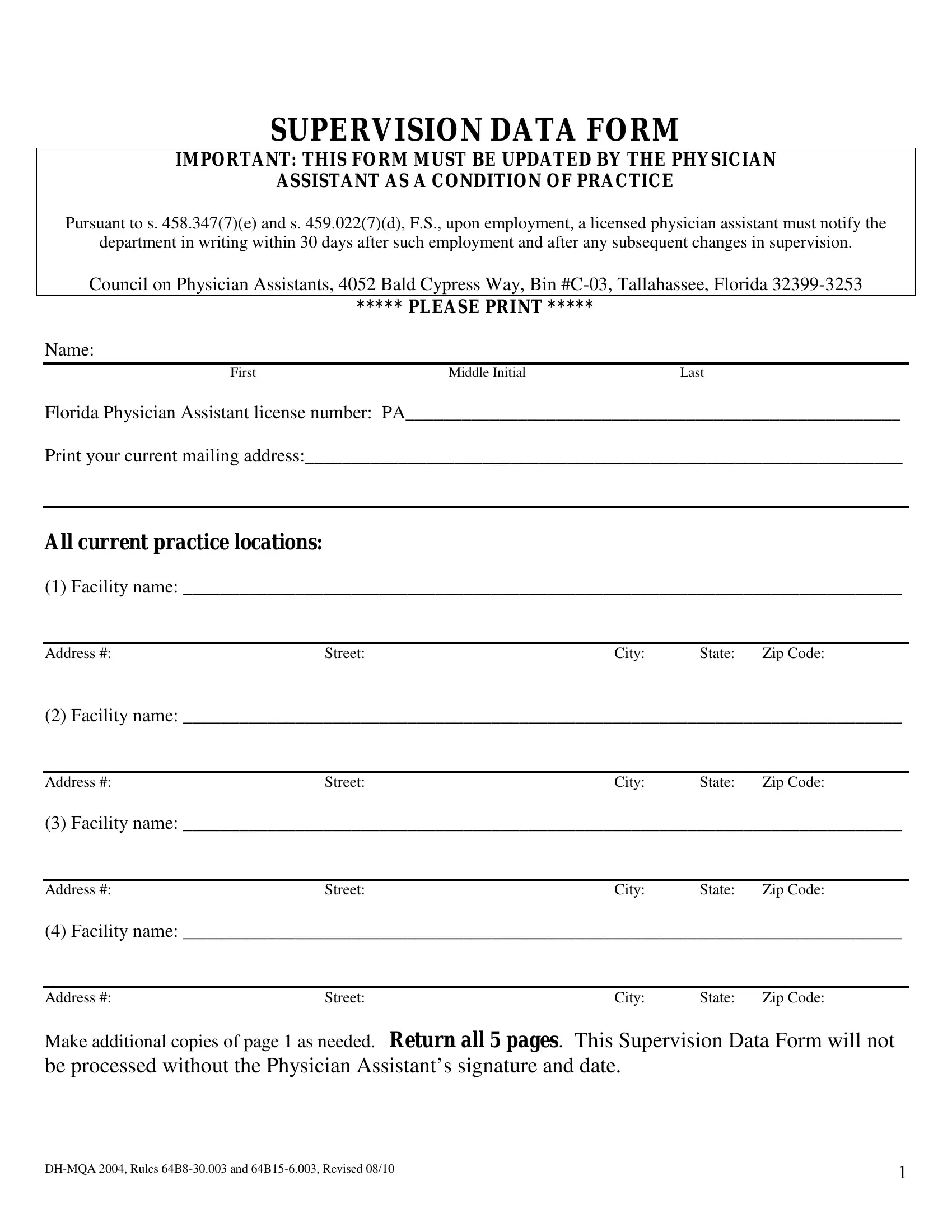
1. The florida physician assistant supervision form involves certain information to be inserted. Ensure the following fields are finalized:
2. Once your current task is complete, take the next step – fill out all of these fields - Address Facility name, Street City State Zip Code, Address Facility name, Street City State Zip Code, Address Make additional copies of, and Street City State Zip Code with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Completing physician, Supervision, and ME or DO license number ME or DO is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Always be extremely attentive while completing physician and Supervision, since this is where many people make errors.
4. To go forward, this fourth step requires filling out a few blank fields. Examples include ME or DO license number ME or DO, which you'll find essential to carrying on with this particular form.
5. And finally, this final subsection is precisely what you will have to finish before finalizing the form. The blanks in this instance are the following: Name and license number of, and Effective date of deletion.
Step 3: After proofreading the entries, hit "Done" and you are done and dusted! Right after registering a7-day free trial account here, you will be able to download florida physician assistant supervision form or send it via email at once. The PDF document will also be readily accessible from your personal cabinet with your every modification. FormsPal is invested in the privacy of our users; we make sure that all information handled by our system is kept secure.