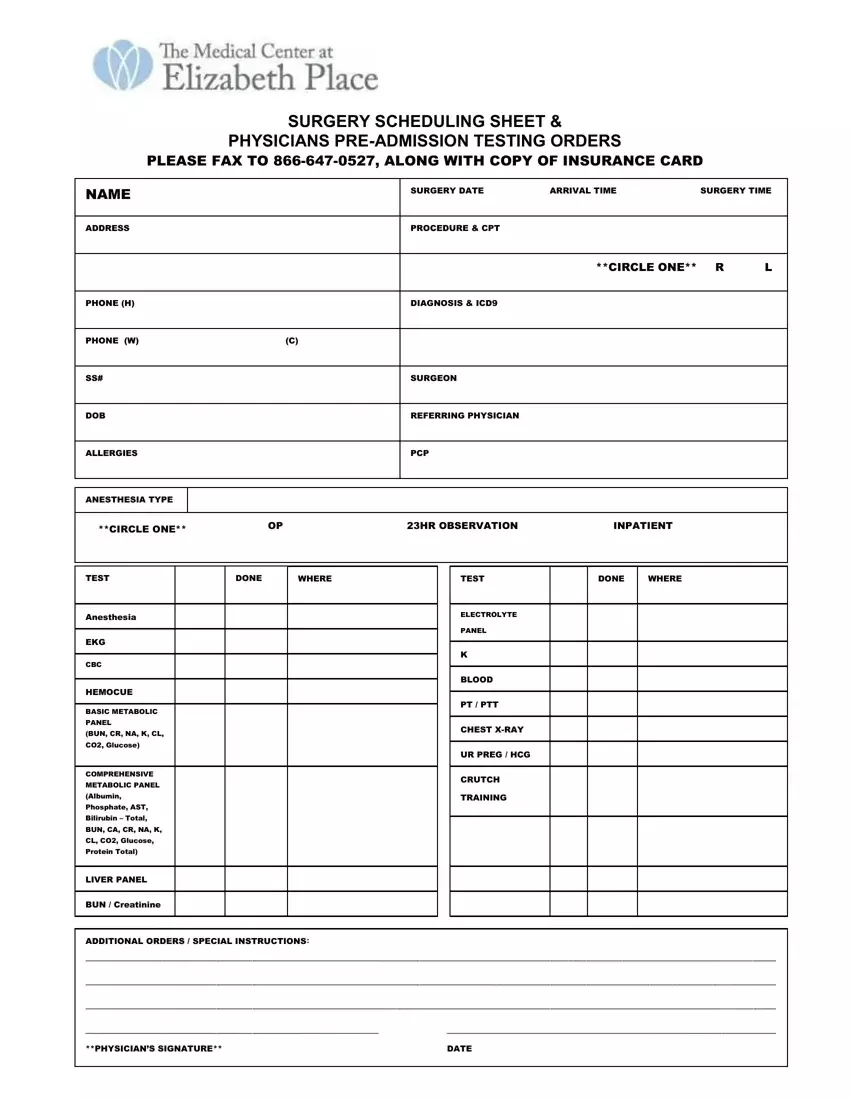
At the heart of modern surgical care, ensuring a seamless and coordinated effort from patient admission to postoperative recovery, lies the comprehensive Surgery Scheduling Sheet & Physicians Pre-Admission Testing Orders form. This critical document, which needs to be faxed to the specified number along with a copy of the insurance card, encompasses all necessary pre-surgical preparations and orders, meticulously detailing everything from patient identification, surgery and arrival times, address, detailed procedure codes, to diagnostic codes and essential contact information. Additionally, it specifies the anesthesia type, various pre-operative tests such as EKG, CBC, and metabolic panels, as well as special instructions for both the patient and medical staff. Beyond the logistics of the scheduled surgery, this form is a gateway to understanding the patient's individual needs, allergies, and potential risks, ensuring that the patient's safety and satisfaction remain paramount. The intention is clear - to foster an environment of individualized care that prioritizes long-term health and patient satisfaction. Patients are guided on how to prepare for the day of surgery, including what to bring, wear, and how to handle preoperative procedures. Information on contacting the Medical Center for financial arrangements and a reminder of the importance of arranging transport post-surgery underline the center’s dedication to patient well-being and safety. This document is not just a formality but a foundational element of patient care, embodying the meticulous planning and coordination necessary to execute a successful surgery.
| Question | Answer |
|---|---|
| Form Name | Surgery Scheduling Sheet |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | surgery scheduling pre, surgery schedule template, sheet medical elizabeth, scheduling sheet pre |
