In the realm of healthcare, particularly within the disciplines concerned with speech and swallowing disorders, the Swallowing Assessment form emerges as an indispensable tool. Crafted thoughtfully to gather comprehensive information, this form delves into various crucial aspects, starting from basic identifiers like the patient's name and ID/medical record number to more detailed inquiries, including the reason for referral and medical diagnosis. Crucial to this evaluation is the history provided by the patient, detailing symptoms such as drooling, coughing, choking, and difficulties swallowing different consistencies, which are pivotal in shaping subsequent therapeutic approaches. Equally important is the documentation of the patient’s current diet and alternative nutrition methods, if any, reflecting a direct link to their swallowing capabilities. The form extends to assess the patient’s self-feeding capacities, mental status, oral motor functions, and even the phonation and respiratory sufficiency, all of which can significantly impact swallowing function. Designed as a resource by the American Speech-Language-Hearing Association (ASHA), it does not just serve as a simple checklist but as a comprehensive guide that aids speech-language pathologists in making informed decisions about the patient’s care plan, embodying a harmonious blend of patient-reported outcomes and objective clinical observations.
| Question | Answer |
|---|---|
| Form Name | Swallowing Assessment Form |
| Form Length | 9 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 15 sec |
| Other names | dysphagia evaluation, swallowing evaluation, clinical bedside swallow evaluation form, bedside swallowing assessment form |
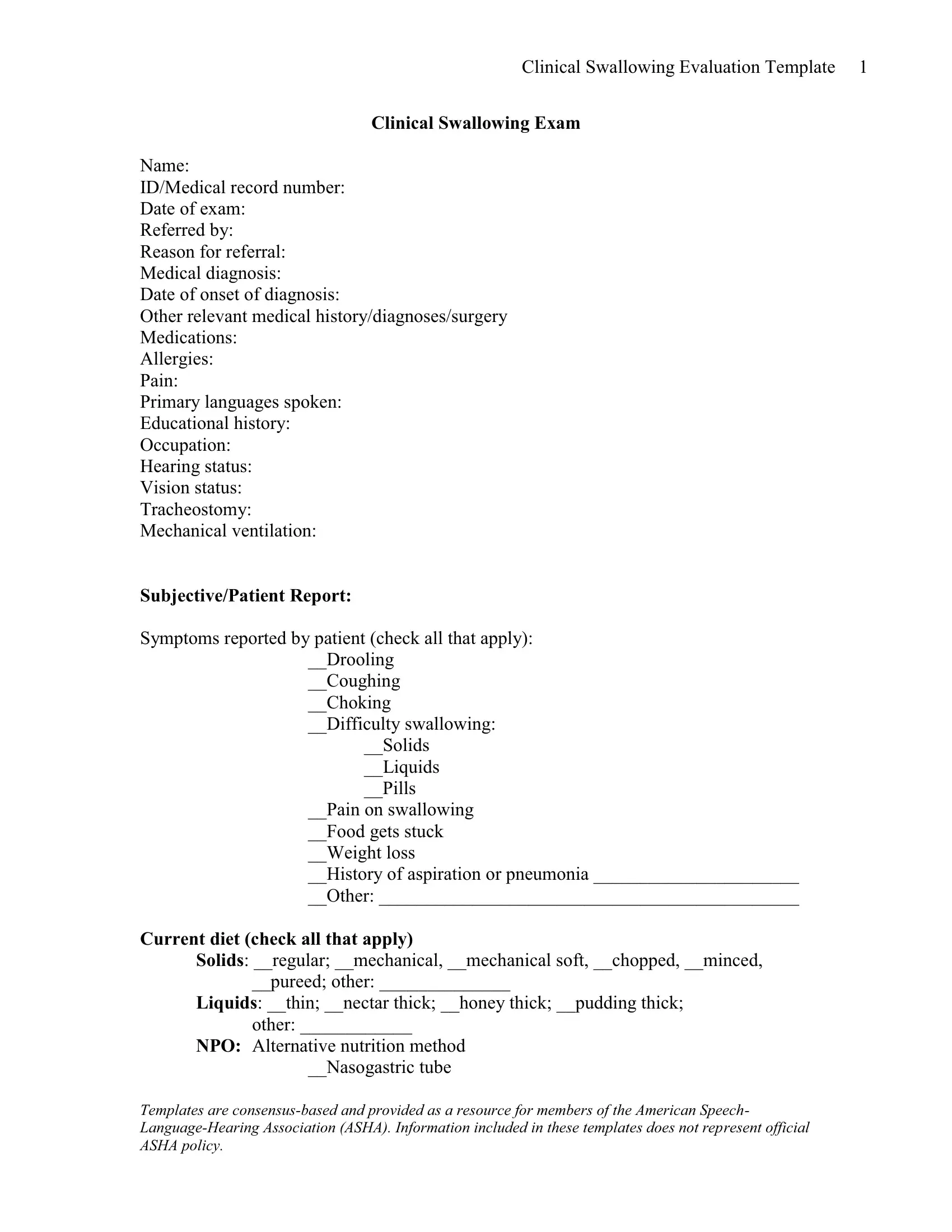
Clinical Swallowing Evaluation Template 1
Clinical Swallowing Exam
Name:
ID/Medical record number:
Date of exam:
Referred by:
Reason for referral:
Medical diagnosis:
Date of onset of diagnosis:
Other relevant medical history/diagnoses/surgery
Medications:
Allergies:
Pain:
Primary languages spoken:
Educational history:
Occupation:
Hearing status:
Vision status:
Tracheostomy:
Mechanical ventilation:
Subjective/Patient Report:
Symptoms reported by patient (check all that apply): __Drooling
__Coughing __Choking __Difficulty swallowing:
__Solids __Liquids __Pills
__Pain on swallowing __Food gets stuck __Weight loss
__History of aspiration or pneumonia ______________________
__Other: _____________________________________________
Current diet (check all that apply)
Solids: __regular; __mechanical, __mechanical soft, __chopped, __minced, __pureed; other: ______________
Liquids: __thin; __nectar thick; __honey thick; __pudding thick; other: ____________
NPO: Alternative nutrition method __Nasogastric tube
Templates are
Clinical Swallowing Evaluation Template 2
__Gastrostomy __Jejunostomy
__Total parenteral nutrition (TPN)
Feeding Method: __Independent in
Endurance during meals: __Good __Fair __Poor __Variable
Observations/Informal Assessment:
Mental Status (check all that apply): __ alert
__ responsive __ cooperative __ confused __ lethargic __ impulsive __ uncooperative __ combative __ unresponsive
Objective Assessment:
Oral Status
Dentition
__WNL
__Missing teeth ________________
__Decay
__Dentures present __upper __lower
Templates are
Clinical Swallowing Evaluation Template 3
Oral Motor, Respiration, and Phonation
Lips
WNL, mild, mod, severe impairment
Observation at rest (WNL, Edema, Erythema, Lesion): __________________
Symmetry, range, speed, strength, tone:
Pucker ______________________________________
Retraction ______________________________________
Alternating pucker/retraction _________________________________
Involuntary movement (e.g., chorea, dystonia, fasciculations, myoclonus, spasms, tremor): __________________________________________________
Tongue
WNL, mild, mod, severe impairment
Observation at rest (WNL, Edema, Erythema, Lesion):
Symmetry, range, speed, strength, tone:
Protrusion _______________________
Retraction _______________________
Lateralization ________________________
Involuntary movement: _______________________
Jaw
WNL, mild, mod, severe impairment
Observation at rest: ____________________
Symmetry, range, strength, tone:
Opening _______________________
Closing ________________________
Lateralization ___________________
Protrusion ______________________
Retraction ______________________
Involuntary movement: _________________
Soft palate
WNL, mild, mod, severe impairment
Observation at rest (WNL, Edema, Erythema, Lesion): ___________________
Symmetry, range, strength, tone: ____________________________________
Elevation _______________________________________________________
Sustained elevation _______________________________________________
Alternating elevation/relaxation _____________________________________
Involuntary movement:
Comments:
Templates are
|
|
|
|
Clinical Swallowing Evaluation Template 4 |
||
Voice quality |
|
|
|
|
|
|
|
|
|
|
|
|
|
Activity |
|
Duration |
Quality |
|
Loudness |
|
|
|
|
|
|
|
|
Phonation |
|
WNL |
WNL |
|
WNL |
|
|
|
Mildly impaired |
Breathy |
|
Reduced |
|
|
|
Moderately impaired |
Hoarse |
|
Excessive |
|
|
|
Severely impaired |
Harsh |
|
|
|
|
|
|
Strained/strangled |
|
|
|
Respiratory Sufficiency and Coordination:
__WNL
__Mildly impaired
__Moderately impaired __Severely impaired
Comments: ________________________________
Food and Liquid Trials
Position during assessment: (check all that apply) __Upright
__Slightly reclined __Fully reclined
Comments: ________________________________
Factors affecting performance:
__No difficulties participating in study
__Impairment or difficulty noted in mental status
__Impairment or difficulty noted in following directions __Impairment or difficulty noted in endurance __Other: __________________________________
Saliva Swallows:
__WNL __Impaired __Xerostomia
Observations: ________________________________
Templates are
Clinical Swallowing Evaluation Template 5
Liquid Trials
Thin Liquids |
|||
Administered |
Administered by |
Administered by |
Administered by |
by (Check all |
(Check all that |
(Check all that |
(Check all that apply) |
that apply) |
apply) |
apply) |
Cup |
Cup |
Cup |
Cup |
Spoon |
Spoon |
Spoon |
Spoon |
Straw |
Straw |
Straw |
Straw |
|
Fed by examiner |
|||
Feeding by |
Fed by examiner |
Fed by examiner |
|
examiner |
|
|
|
Amounts: |
Amounts: |
Amounts: |
Amounts: |
|
|
|
|
Response: |
Response: |
Response: |
Response: |
Volitional cough: |
Volitional cough: |
Volitional cough: |
Volitional cough: |
yes/no |
yes/no |
yes/no |
yes/no |
Volitional throat |
Volitional throat |
Volitional throat |
Volitional throat clear: |
clear: yes/no |
clear: yes/no |
clear: yes/no |
yes/no |
Spontaneous |
Spontaneous |
Spontaneous |
Spontaneous cough |
cough during |
cough during |
cough during |
during trials: yes/no |
trials: yes/no |
trials: yes/no |
trials: yes/no |
Spontaneous throat |
Spontaneous |
Spontaneous throat |
Spontaneous throat |
clear during trials: |
throat clear |
clear during |
clear during |
yes/no |
during trials: |
trials: yes/no |
trials: yes/no |
|
yes/no |
|
|
|
Strategies |
Strategies |
Strategies |
Strategies Attempted |
Attempted and |
Attempted and |
Attempted and |
and Response: |
Response: |
Response: |
Response: |
|
|
|
|
|
Swallowing |
Swallowing |
Swallowing |
Swallowing Duration |
Duration |
Duration |
Duration |
___ sec. |
(introduction of |
___ sec. |
___ sec. |
|
bolus to |
|
|
|
completion of |
|
|
|
pharyngeal |
|
|
|
stage): ___sec. |
|
|
|
Comments __________________________________________________
Templates are
Clinical Swallowing Evaluation Template 6
Solid Food Trials
Food Item: |
Food Item: |
Food Item: |
Food Item: |
|
|
|
|
Administered |
Spoon/fork |
Spoon/fork |
Spoon/fork |
by: |
|||
Spoon/fork |
Fed by examiner |
Fed by examiner |
Fed by examiner |
|
|
|
|
Fed by examiner |
|
|
|
Amounts: |
Amounts: |
Amounts: |
Amounts: |
|
|
|
|
Response: |
Response: |
Response: |
Response: |
(circle all that |
|
(check all that |
(check all that apply) |
apply) |
|
apply) |
Volitional cough: |
Volitional cough: |
Volitional cough: |
Volitional cough: |
yes/no |
yes/no |
yes/no |
yes/no |
Volitional throat clear: |
Volitional throat |
Volitional throat |
Volitional throat |
yes/no |
clear: yes/no |
clear: yes/no |
clear: yes/no |
Spontaneous cough |
Spontaneous |
Spontaneous |
Spontaneous |
during trials: yes/no |
cough during |
cough during |
cough during |
Spontaneous throat |
trials: yes/no |
trials: yes/no |
trials: yes/no |
clear during trials: |
Spontaneous |
Spontaneous throat |
Spontaneous throat |
yes/no |
throat clear |
clear during |
clear during |
|
during trials: |
trials: yes/no |
trials: yes/no |
|
yes/no |
|
|
|
Strategies |
Strategies |
Strategies |
Strategies Attempted |
Attempted and |
Attempted and |
Attempted and |
and Response: |
Response: |
Response: |
Response: |
|
Swallowing |
Swallowing |
Swallowing |
Swallowing Duration |
Duration |
Duration |
Duration |
___ sec. |
(introduction of |
___ sec. |
___ sec. |
|
bolus to |
|
|
|
completion of |
|
|
|
pharyngeal |
|
|
|
stage): ___sec. |
|
|
|
Observations: (laryngeal elevation, other)
________________________________________________________________________
________________________________________________________________________
Templates are
Clinical Swallowing Evaluation Template 7
Findings
__Swallowing within normal limits __Swallowing diagnosis:
__dysphagia unspecified __oral phase dysphagia __oropharyngeal phase dysphagia __pharyngeal phase dysphagia
__pharyngoesophageal phase dysphagia __other dysphagia
__Severity: __mild
Characterized by: ______________________________________________________
Contributing Factors to Swallowing Impairment __Reduced alertness or attention __Difficulty following directions __Reduced oral strength/coordination/sensation __Mastication inefficiency
__Impaired
__Impaired velopharyngeal closure/coordination __Delayed swallow initiation
__Reduced laryngeal excursion
__Other ___________________________________
Prognosis: __Good __Fair __ Poor, based on ________________________
Impact on Safety and Functioning (check all that apply) __No limitations
__Risk for aspiration: ______________________________
__Risk for inadequate nutrition/hydration: ______________________________
NOMS Swallowing Score
Templates are
Clinical Swallowing Evaluation Template 8
Recommendations:
Instrumental assessment: __yes __no
__Videofluoroscopic Swallowing Study __Endoscopic Swallowing Study
Swallowing treatment: __yes __no
Frequency: Duration:
Diet Texture Recommendations:
Solids: __regular; __mechanical, __mechanical soft, __chopped, __minced, __pureed; other: ______________
Liquids: __thin; __nectar thick; __honey thick; __pudding thick; other: ____________
NPO with alternative nutrition method: ____________________________
Alternative nutrition method with pleasure feedings: _________________
Other: _______________________________________
Safety precautions/swallowing recommendations (check all that apply): __Supervision needed for all meals
__1 to 1 close supervision __1 to 1 distant supervision
__To be fed only by trained staff/family __To be fed only by SLP
__Feed only when alert __Reduce distractions
__Needs verbal cues to use recommended strategies __Upright position at least 30 minutes after meals __Small sips and bites when eating
__Slow rate; swallow between bites __No straw
__Sips by straw only
__Multiple swallows: ____________________
__Alternate liquids and solids
__Sensory enhancement (flavor, texture, temperature): ______________
__Other _________________________
Other recommended referrals: __Dietetics __Gastroenterology __Neurology __Otolaryngology __Pulmonology
__Other _________________________
Templates are
Clinical Swallowing Evaluation Template 9
Patient/Caregiver Education __Described results of evaluation
__Patient expressed understanding of evaluation and agreement with goals and treatment plan
__Family/caregivers expressed understanding of evaluation and agreement with goals and treatment plan.
__ Patient expressed understanding of safety precautions/feeding recommendations
__ Family/caregivers expressed understanding of safety precautions/feeding recommendations
__Patient expressed understanding of evaluation but refused treatment __ Patient requires further education
__Family/caregivers require further education
Treatment Plan
Long Term Goals
Short Term Goals
Templates are