
insurance statement proof of can be filled out without any problem. Simply open FormsPal PDF editing tool to complete the job promptly. FormsPal team is dedicated to giving you the perfect experience with our editor by regularly presenting new capabilities and improvements. Our editor has become even more helpful with the most recent updates! So now, working with PDF forms is a lot easier and faster than ever. Getting underway is easy! Everything you should do is follow the next basic steps below:
Step 1: Access the PDF file in our tool by pressing the "Get Form Button" at the top of this page.
Step 2: This editor helps you modify nearly all PDF forms in a range of ways. Modify it by writing any text, correct original content, and add a signature - all at your convenience!
In an effort to fill out this document, ensure you provide the right details in each and every blank field:
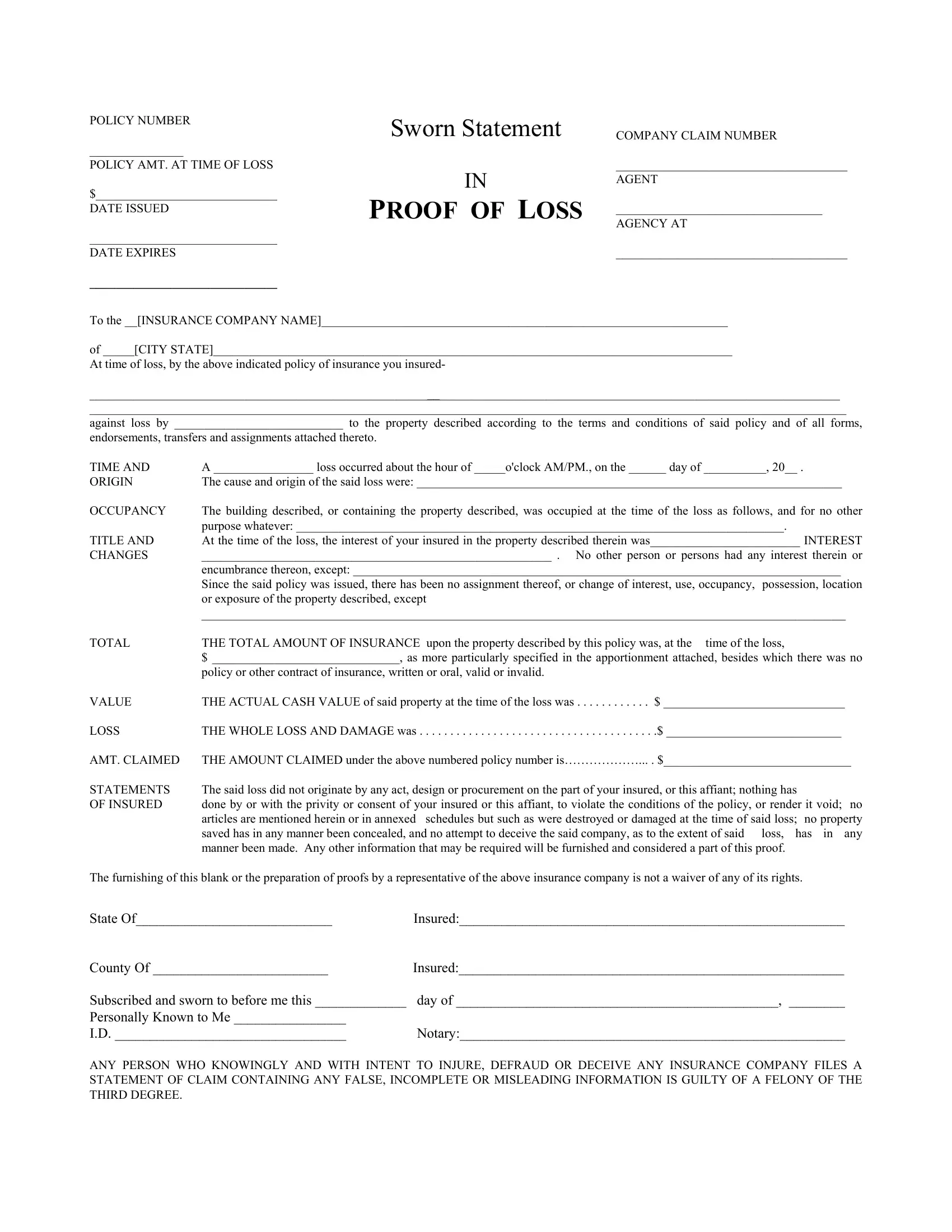
1. For starters, while filling out the insurance statement proof of, begin with the section that has the following blanks:
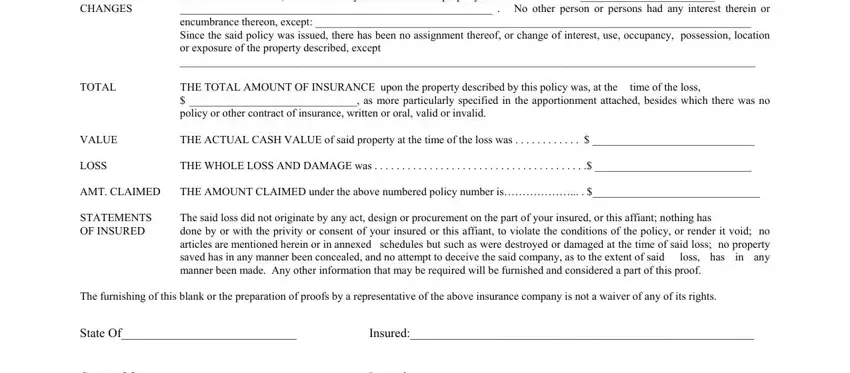
2. Just after filling out the previous step, head on to the subsequent part and fill in the necessary details in these fields - POLICY NUMBER POLICY AMT AT TIME, The building described or, time of the loss, THE WHOLE LOSS AND DAMAGE was, loss has, and THE ACTUAL CASH VALUE of said.
3. Through this stage, review POLICY NUMBER POLICY AMT AT TIME, and ANY PERSON WHO KNOWINGLY AND WITH. These need to be completed with greatest accuracy.
Those who use this document generally get some points wrong while filling out ANY PERSON WHO KNOWINGLY AND WITH in this part. Don't forget to review what you enter here.
Step 3: Make certain the information is right and simply click "Done" to proceed further. Obtain your insurance statement proof of after you sign up for a 7-day free trial. Easily gain access to the document within your personal account, along with any modifications and changes being automatically saved! Here at FormsPal, we strive to make sure all your information is maintained private.