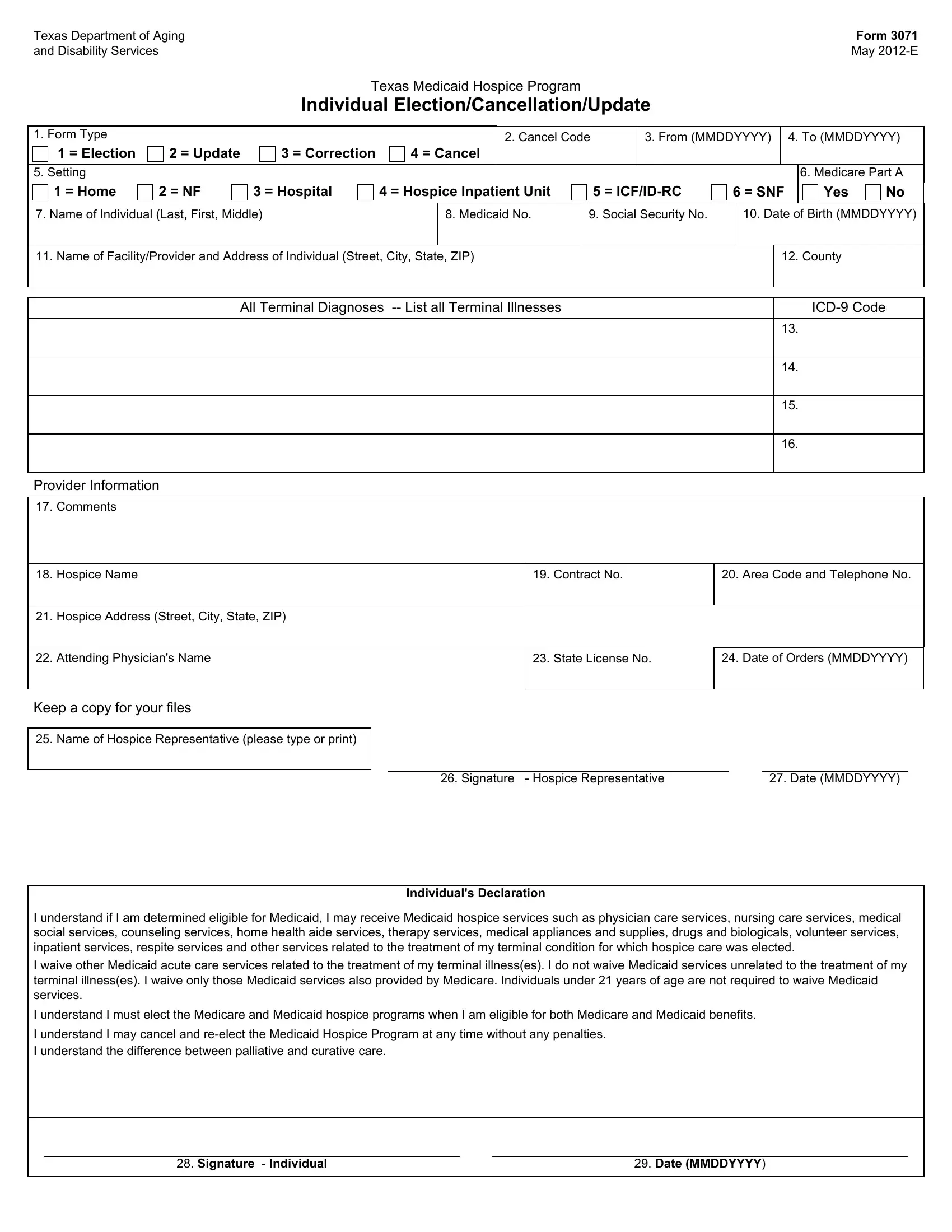
In the evolving landscape of healthcare, the Texas Department of Aging and Disability Services has introduced the Texas 3071 form, a crucial document for residents navigating the complexities of Medicaid hospice care since May 2012. This form serves multiple functions, including the election, cancellation, or updating of an individual's decision to receive hospice care under the Texas Medicaid Hospice Program. With options to denote the setting of care ranging from home to various facility types and the inclusion of Medicare Part A status, the form meticulously gathers essential information. It requires the individual's personal details alongside the Medicaid and Social Security numbers, ensuring a comprehensive approach to their care. Facility or provider information, complete with terminal diagnoses listed with ICD-9 codes, foregrounds the medical context. Moreover, the form details the hospice provider's information, reinforcing the partnership in care. Notably, it emphasizes patient autonomy and informed consent through the individual's declaration, which articulates an understanding of the hospice services covered, the waiver of certain Medicaid acute care services in favor of palliative care, and the rights regarding the cancellation and re-election of the service. This document highlights the intricate balance between regulatory requirements and the personalized needs of individuals facing terminal illnesses, ensuring they receive dignified and tailored care. The Texas 3071 form stands as a testament to a structured yet flexible approach to end-of-life care, placing individuals' preferences and welfare at the forefront.
| Question | Answer |
|---|---|
| Form Name | Texas Form 3071 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | medicaid, printable texas medicaid application form, Entiendo, hospicio |
