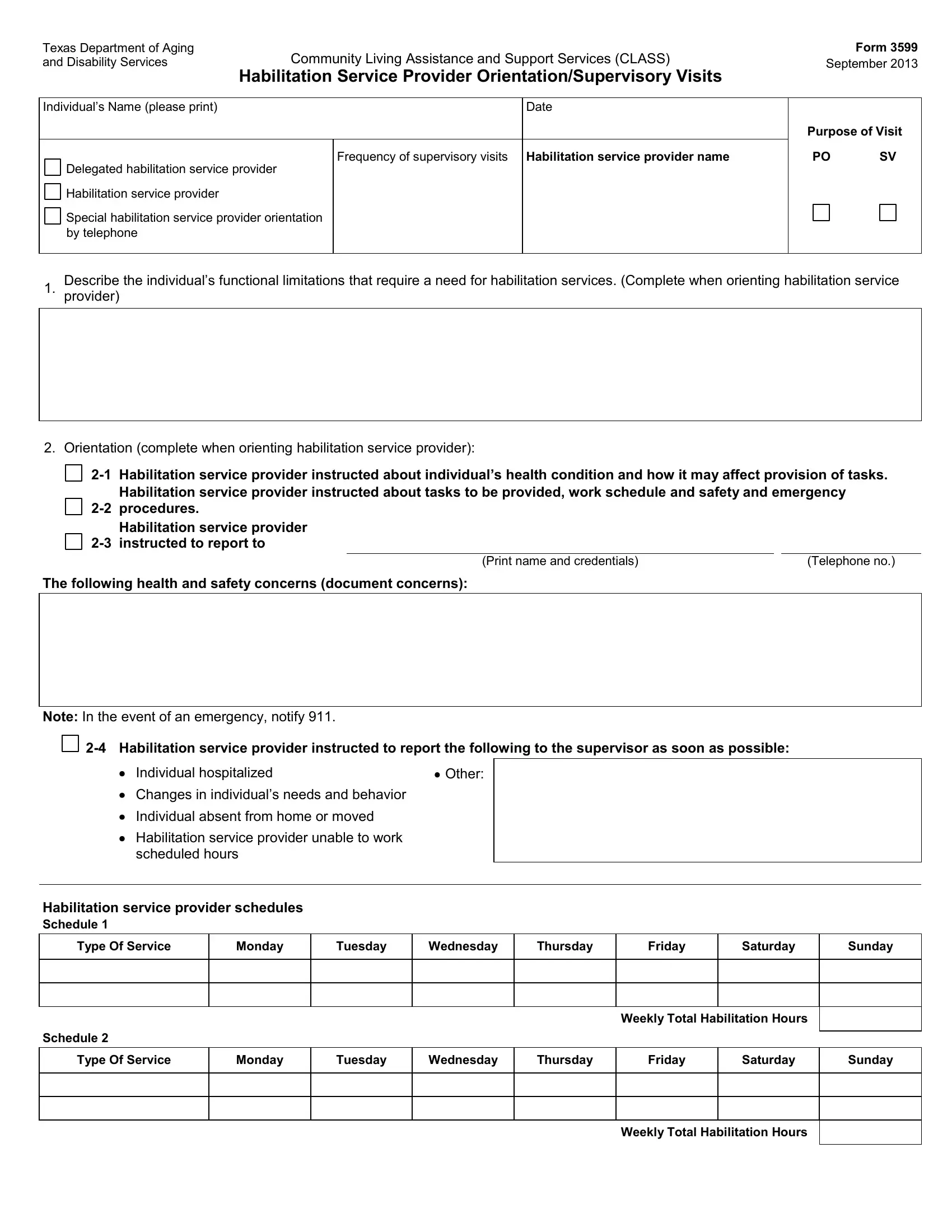
In the intricate world of care and assistance for individuals with disabilities, the Texas Department of Aging and Disability Services plays a crucial role, especially through its CLASS program which stands for Community Living Assistance and Support Services. Key to the effective implementation of this program is the Texas 3599 form, a document designed to ensure that habilitation service providers are thoroughly oriented and supervised in their roles. Introduced in September 2013, this form encompasses a comprehensive overview of an individual’s needs, detailing their functional limitations, the specific habilitation services required, and the frequency of supervisory visits necessary to monitor the quality of care provided. Moreover, it serves as a critical tool for recording the orientation of new service providers, ensuring they are fully instructed on the health condition of the individual they're supporting, the tasks they must perform, their work schedule, and essential safety and emergency procedures. The form also mandates the reporting of any significant changes in the individual’s condition or needs, alongside detailing the habilitation service provider’s responsibilities in emergency situations. Through schedules, it meticulously outlines the weekly total of habilitation hours allocated per service type, ensuring a structured approach to care delivery. Additionally, it assesses the provider's competency in delivering both habilitation and medically related tasks, while also capturing feedback from the individual or their legally authorized representative (LAR) on the satisfaction and effectiveness of the services rendered. The form closes with an evaluation of the ongoing need for services and invites additional comments, thereby providing a holistic snapshot of the care process from orientation to ongoing supervision.
| Question | Answer |
|---|---|
| Form Name | Texas Form 3599 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Texas, you form 3599, orientation supervisory visits, 2012 |
