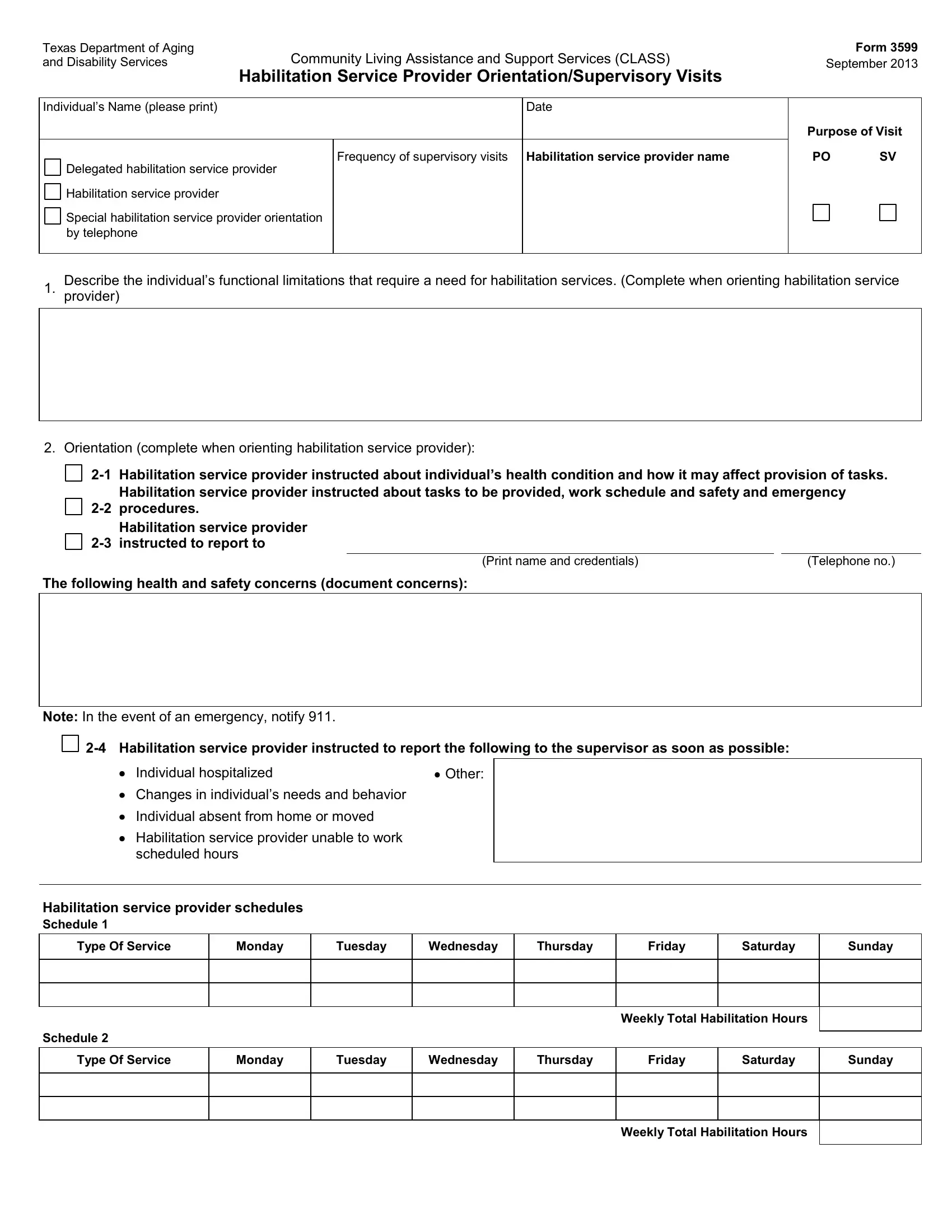
In the intricate world of care and assistance for individuals with disabilities, the Texas Department of Aging and Disability Services plays a crucial role, especially through its CLASS program which stands for Community Living Assistance and Support Services. Key to the effective implementation of this program is the Texas 3599 form, a document designed to ensure that habilitation service providers are thoroughly oriented and supervised in their roles. Introduced in September 2013, this form encompasses a comprehensive overview of an individual’s needs, detailing their functional limitations, the specific habilitation services required, and the frequency of supervisory visits necessary to monitor the quality of care provided. Moreover, it serves as a critical tool for recording the orientation of new service providers, ensuring they are fully instructed on the health condition of the individual they're supporting, the tasks they must perform, their work schedule, and essential safety and emergency procedures. The form also mandates the reporting of any significant changes in the individual’s condition or needs, alongside detailing the habilitation service provider’s responsibilities in emergency situations. Through schedules, it meticulously outlines the weekly total of habilitation hours allocated per service type, ensuring a structured approach to care delivery. Additionally, it assesses the provider's competency in delivering both habilitation and medically related tasks, while also capturing feedback from the individual or their legally authorized representative (LAR) on the satisfaction and effectiveness of the services rendered. The form closes with an evaluation of the ongoing need for services and invites additional comments, thereby providing a holistic snapshot of the care process from orientation to ongoing supervision.
| Question | Answer |
|---|---|
| Form Name | Texas Form 3599 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Texas, you form 3599, orientation supervisory visits, 2012 |
Texas Department of Aging |
Community Living Assistance and Support Services (CLASS) |
|
and Disability Services |
|
|
|
Habilitation Service Provider Orientation/Supervisory Visits |
|
|
|
|
Individual’s Name (please print) |
Date |
|
|
|
|
|
Frequency of supervisory visits Habilitation service provider name |
|
Delegated habilitation service provider |
|
|
Habilitation service provider |
|
|
Special habilitation service provider orientation by telephone
Form 3599
September 2013
Purpose of Visit
PO SV
Describe the individual’s functional limitations that require a need for habilitation services. (Complete when orienting habilitation service
1. provider)
2. Orientation (complete when orienting habilitation service provider):
Habilitation service provider instructed about individual’s health condition and how it may affect provision of tasks. |
||||
|
Habilitation service provider instructed about tasks to be provided, work schedule and safety and emergency |
|||
procedures. |
|
|
||
|
Habilitation service provider |
|
|
|
instructed to report to |
|
|
||
|
|
|
|
|
|
|
(Print name and credentials) |
|
(Telephone no.) |
The following health and safety concerns (document concerns):
Note: In the event of an emergency, notify 911.
Individual hospitalized |
Other: |
Changes in individual’s needs and behavior
Individual absent from home or moved
Habilitation service provider unable to work scheduled hours
Habilitation service provider schedules
Schedule 1
Type Of Service |
Monday |
Tuesday |
Wednesday |
Thursday |
Friday |
Saturday |
Sunday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weekly Total Habilitation Hours
Schedule 2
Type Of Service
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday
Weekly Total Habilitation Hours
Form 3599
Page 2 /
Individual’s Name (please print)
3.A. Tasks/Plan of Care: Indicate tasks to be performed (complete on every visit). During supervisory visit, ask individual or LAR what tasks are provided by the service provider. Observe or ask about performance: S = Satisfactory U = Unsatisfactory
Hygiene..............
Toileting.............
Dressing.............
Shopping ...........
Meal Preparation
Freq. Perform.
Feeding ..........................
Exercise .........................
Transfer/Ambulation......
Cleaning .........................
Community Assistance
Freq. Perform.
Medically Related Tasks......
Freq. Perform.
3.B. Is the habilitation service provider competent to provide habilitation tasks? |
Yes |
|
|
3.C. Is the habilitation service provider competent to provide delegated habilitation tasks? |
Yes |
|
3.D. Is the habilitation service provider competent to provide medically related tasks? |
Yes |
Complete the following for Supervisory Visits (N/A for habilitation service provider orientation only).
4. |
Is the individual satisfied with the services provided by the habilitation service provider? |
Yes |
|
||
5. |
Is the habilitation service provider following the schedule? |
Yes |
6.A. |
Describe service delivery problems. |
|
No
No
No
No No
N/A
N/A
N/A
6.B. Describe habilitation service provider training needs.
6.C. Describe corrective actions taken.
7. Does the individual continue to need services? ...........................................................................................................
8. Additional Comments:
Yes
No
Signature – Individual/LAR |
|
Date |
|
|
|
Signature – Habilitation Service Provider |
|
Date |
|
|
|
Signature – Supervisor |
|
Date |