
You are able to work with Texas From Dl 77 Form effectively using our PDFinity® PDF editor. To make our tool better and simpler to work with, we consistently implement new features, bearing in mind feedback coming from our users. With just several basic steps, you may begin your PDF journey:
Step 1: Hit the orange "Get Form" button above. It'll open our pdf editor so that you can begin completing your form.
Step 2: When you start the PDF editor, you will get the form prepared to be filled in. Besides filling in different fields, you could also do many other things with the form, such as putting on your own text, changing the initial text, adding illustrations or photos, putting your signature on the form, and much more.
When it comes to blanks of this precise PDF, here's what you want to do:
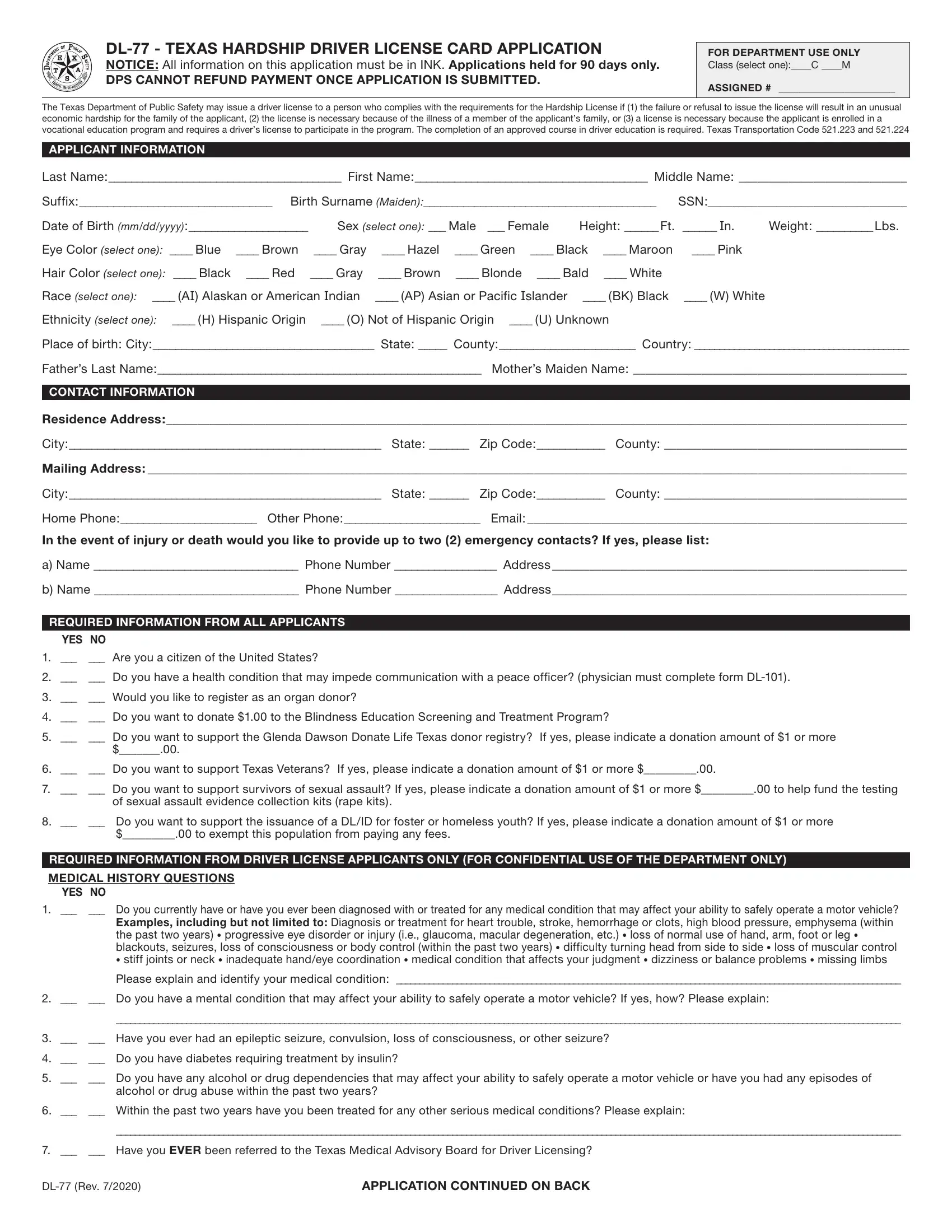
1. It is recommended to fill out the Texas From Dl 77 Form correctly, therefore pay close attention when working with the sections containing these blanks:
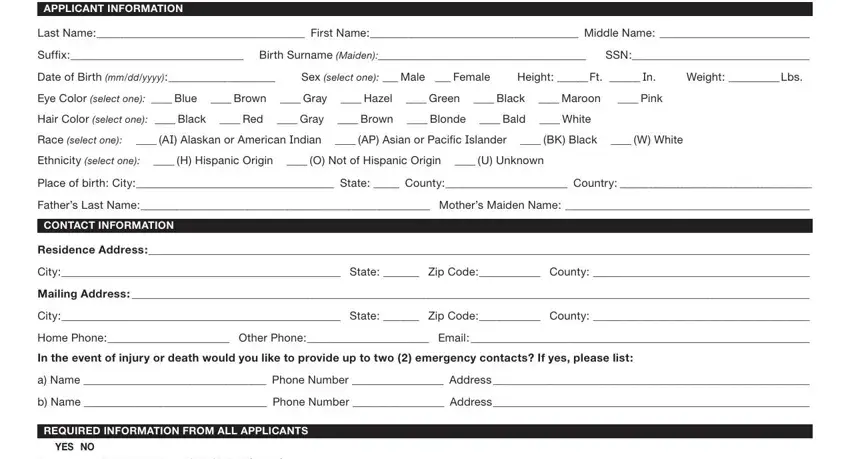
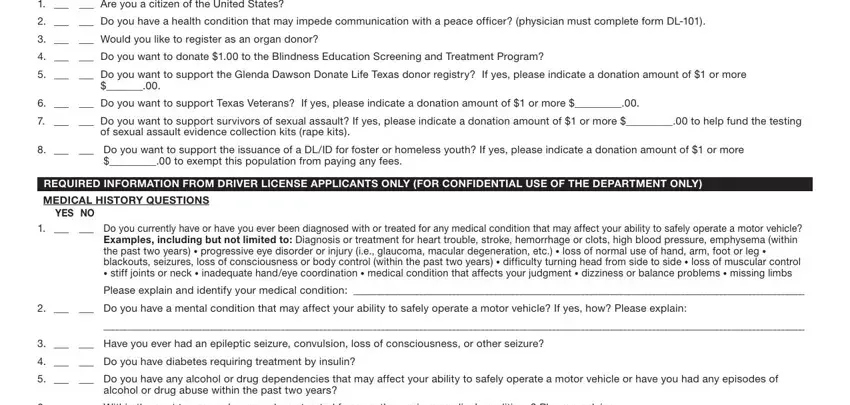
2. Soon after the prior array of blanks is done, proceed to enter the applicable details in all these: Are you a citizen of the United, Do you have a health condition, Would you like to register as, Do you want to donate to the, Do you want to support the, Do you want to support Texas, Do you want to support, of sexual assault evidence, Do you want to support the, to exempt this population from, REQUIRED INFORMATION FROM DRIVER, MEDICAL HISTORY QUESTIONS, YES NO, Do you currently have or have, and Please explain and identify your.
A lot of people often make some mistakes while filling out Do you want to support in this area. Be certain to reread whatever you type in here.
3. The following step is all about Within the past two years have, Have you EVER been referred to, DL Rev, and APPLICATION CONTINUED ON BACK - fill in each one of these empty form fields.

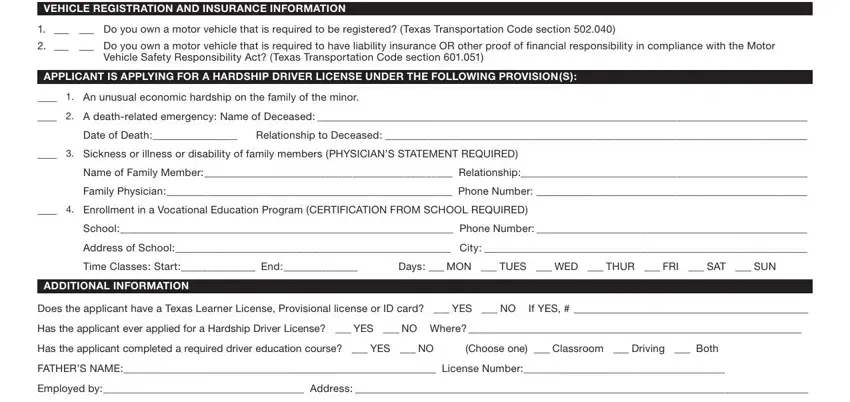
4. The form's fourth section comes next with the next few fields to focus on: VEHICLE REGISTRATION AND INSURANCE, Do you own a motor vehicle that, Do you own a motor vehicle that, Vehicle Safety Responsibility Act, APPLICANT IS APPLYING FOR A, An unusual economic hardship on, A deathrelated emergency Name of, Date of Death Relationship to, Sickness or illness or, Name of Family Member Relationship, Family Physician Phone Number, Enrollment in a Vocational, School Phone Number, Address of School City, and Time Classes Start End Days MON.
5. The form needs to be wrapped up with this area. Below you'll find a comprehensive set of fields that require appropriate information for your document usage to be accomplished: Work Hours Work Phone, MOTHERS NAME License Number, Employed by Address, Work Hours Work Phone, List all other members of the, Name License Relationship, Name License Relationship, Name License Relationship, Explain all necessary driving of, Use extra page if necessary, Texas law requires the Texas, I hereby acknowledge receipt of, Minor Applicant, ParentLegal Guardian, and Date of Receipt.
Step 3: Make sure that the details are correct and simply click "Done" to proceed further. Acquire the Texas From Dl 77 Form the instant you register online for a 7-day free trial. Easily get access to the pdf document in your FormsPal account, along with any modifications and adjustments conveniently synced! FormsPal provides safe document editing devoid of personal information record-keeping or distributing. Be assured that your data is safe here!