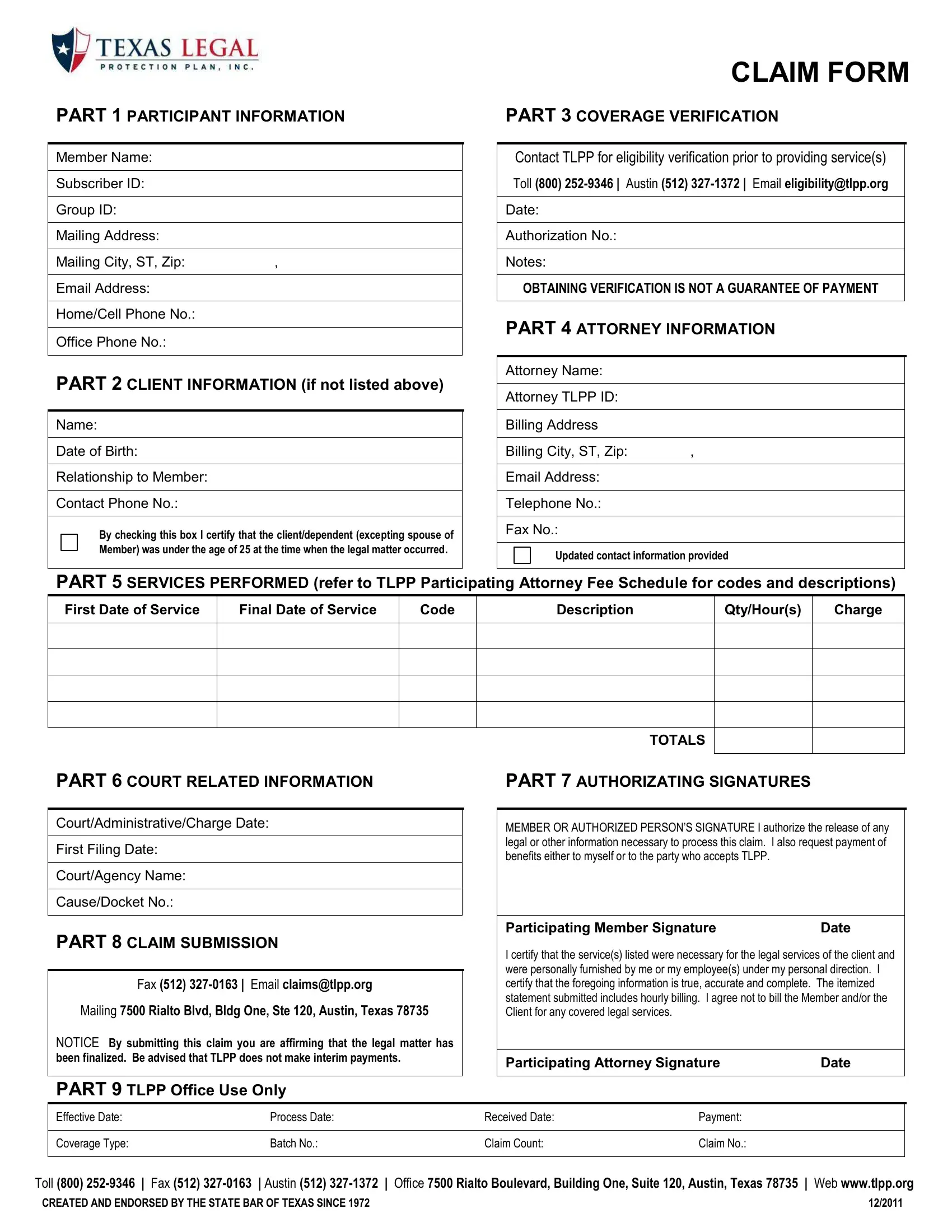
Navigating the complexities of legal claims in Texas can seem daunting, especially for those unfamiliar with the process. However, the Texas Legal Claim form is designed to streamline the submission of legal claims for individuals seeking legal assistance. This comprehensive form encompasses several critical parts, beginning with the Participant Information section, where the member's personal details, such as name, subscriber ID, group ID, and contact information, are gathered. It also provides space for Client Information, should the service be intended for someone other than the member, including details like name, date of birth, and relationship to the member. A critical aspect of the form is the Coverage Verification part, reminding individuals to contact the Texas Legal Protection Plan (TLPP) to verify eligibility before any legal service is rendered, although it's noted that obtaining verification doesn't guarantee payment. Further, the form requests detailed Attorney Information, ensuring that the attorney is registered with TLPP and their contact information is up to date. The Services Performed section allows for the listing of services provided, in line with the TLPP Participating Attorney Fee Schedule, while Court Related Information captures essential details about legal proceedings. Additionally, the Claim Submission notice emphasizes the crucial point that TLPP does not make interim payments and that submission signifies the legal matter's conclusion. Lastly, the form concludes with sections for Authorizing Signatures from both the member (or authorized person) and the participating attorney, affirming the accuracy of the information provided and the necessity of the services rendered. With such a structured approach, the Texas Legal Claim form aims to simplify the legal claims process, ensuring that members have a clear path to follow when seeking legal assistance through TLPP. Created and endorsed by the State Bar of Texas, this form is a testament to the commitment to providing structured legal support to its members.
| Question | Answer |
|---|---|
| Form Name | Texas Legal Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Qty, AUTHORIZATING, affirming, 1972 |
PART 1 PARTICIPANT INFORMATION
Member Name:
Subscriber ID:
Group ID:
Mailing Address:
Mailing City, ST, Zip: |
, |
|
|
Email Address: |
|
|
|
Home/Cell Phone No.: |
|
|
|
Office Phone No.: |
|
|
|
PART 2 CLIENT INFORMATION (if not listed above)
Name:
Date of Birth:
Relationship to Member:
Contact Phone No.:
By checking this box I certify that the client/dependent (excepting spouse of Member) was under the age of 25 at the time when the legal matter occurred.
CLAIM FORM
PART 3 COVERAGE VERIFICATION
Contact TLPP for eligibility verification prior to providing service(s)
Toll (800)
Date:
Authorization No.:
Notes:
OBTAINING VERIFICATION IS NOT A GUARANTEE OF PAYMENT
PART 4 ATTORNEY INFORMATION
Attorney Name:
Attorney TLPP ID:
Billing Address
Billing City, ST, Zip: ,
Email Address:
Telephone No.:
Fax No.:
Updated contact information provided
PART 5 SERVICES PERFORMED (refer to TLPP Participating Attorney Fee Schedule for codes and descriptions)
First Date of Service
Final Date of Service
Code
Description
Qty/Hour(s)
Charge
TOTALS
PART 6 COURT RELATED INFORMATION
Court/Administrative/Charge Date:
First Filing Date:
Court/Agency Name:
Cause/Docket No.:
PART 8 CLAIM SUBMISSION
Fax (512)
Mailing 7500 Rialto Blvd, Bldg One, Ste 120, Austin, Texas 78735
NOTICE By submitting this claim you are affirming that the legal matter has been finalized. Be advised that TLPP does not make interim payments.
PART 7 AUTHORIZATING SIGNATURES
MEMBER OR AUTHORIZED PERSON’S SIGNATURE I authorize the release of any legal or other information necessary to process this claim. I also request payment of benefits either to myself or to the party who accepts TLPP.
Participating Member Signature |
Date |
I certify that the service(s) listed were necessary for the legal services of the client and were personally furnished by me or my employee(s) under my personal direction. I certify that the foregoing information is true, accurate and complete. The itemized statement submitted includes hourly billing. I agree not to bill the Member and/or the Client for any covered legal services.
Participating Attorney Signature |
Date |
PART 9 TLPP Office Use Only
Effective Date: |
Process Date: |
Received Date: |
Payment: |
|
|
|
|
Coverage Type: |
Batch No.: |
Claim Count: |
Claim No.: |
|
|
|
|
Toll (800) |
Web www.tlpp.org |
CREATED AND ENDORSED BY THE STATE BAR OF TEXAS SINCE 1972 |
12/2011 |