For individuals and healthcare providers navigating the complexities of obtaining initial outpatient therapy services within the Children with Special Health Care Needs (CSHCN) Services Program in Texas, the Authorization Request for Initial Outpatient Therapy (TP1) form emerges as a vital document. Designed to streamline the authorization process for physical therapy (PT), occupational therapy (OT), and speech-language pathology (SLP) services, this form mandates comprehensive completion to avoid denial of claims. Clinicians and authorized representatives are advised to download the most current version from the Texas Medicaid & Healthcare Partnership (TMHP) website, ensuring that all client and provider information, along with specific service requests and necessary evaluations, are accurately detailed. The form underscores the importance of attaching evaluation summaries and clearly defining the required services, including procedure codes, service dates, and frequency of sessions. It also intricately details the submission process, either via mail or fax, and highlights the significance of direct contact with the TMHP-CSHCN Services Program for assistance, thus emphasizing the collaborative effort required to facilitate these essential health care services for eligible clients.
| Question | Answer |
|---|---|
| Form Name | Texas Medicaid Tp 1 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | initial tp1 forms, how to tp1 forms, medicaid tp1 form, tp1e5c743d573148e021080 |
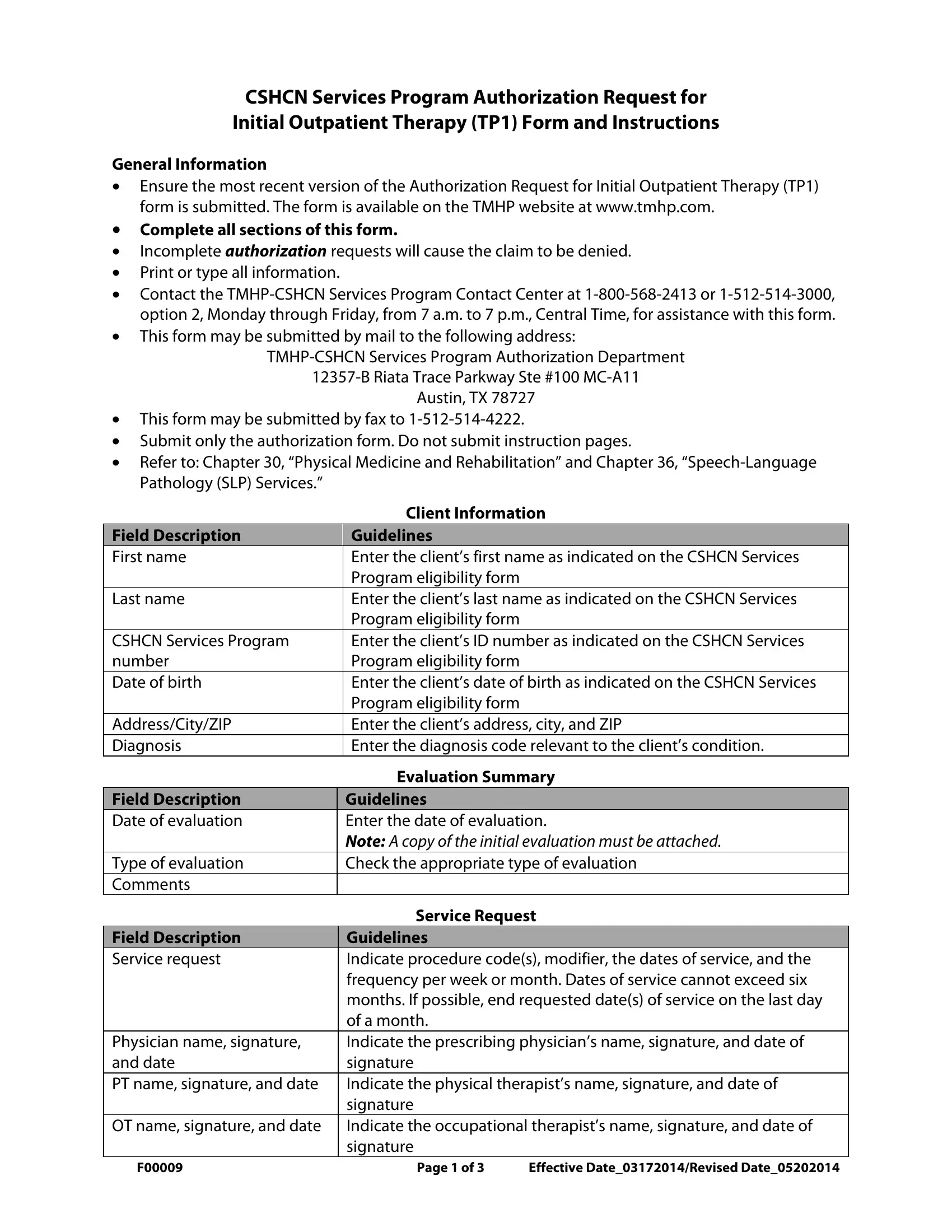
CSHCN Services Program Authorization Request for
Initial Outpatient Therapy (TP1) Form and Instructions
General Information
•Ensure the most recent version of the Authorization Request for Initial Outpatient Therapy (TP1) form is submitted. The form is available on the TMHP website at www.tmhp.com.
•Complete all sections of this form.
•Incomplete authorization requests will cause the claim to be denied.
•Print or type all information.
•Contact the
•This form may be submitted by mail to the following address:
Austin, TX 78727
•This form may be submitted by fax to
•Submit only the authorization form. Do not submit instruction pages.
•Refer to: Chapter 30, “Physical Medicine and Rehabilitation” and Chapter 36,
|
Client Information |
Field Description |
Guidelines |
First name |
Enter the client’s first name as indicated on the CSHCN Services |
|
Program eligibility form |
Last name |
Enter the client’s last name as indicated on the CSHCN Services |
|
Program eligibility form |
CSHCN Services Program |
Enter the client’s ID number as indicated on the CSHCN Services |
number |
Program eligibility form |
Date of birth |
Enter the client’s date of birth as indicated on the CSHCN Services |
|
Program eligibility form |
Address/City/ZIP |
Enter the client’s address, city, and ZIP |
Diagnosis |
Enter the diagnosis code relevant to the client’s condition. |
|
Evaluation Summary |
Field Description |
Guidelines |
Date of evaluation |
Enter the date of evaluation. |
|
Note: A copy of the initial evaluation must be attached. |
Type of evaluation |
Check the appropriate type of evaluation |
Comments |
|
|
Service Request |
Field Description |
Guidelines |
Service request |
Indicate procedure code(s), modifier, the dates of service, and the |
|
frequency per week or month. Dates of service cannot exceed six |
|
months. If possible, end requested date(s) of service on the last day |
|
of a month. |
Physician name, signature, |
Indicate the prescribing physician’s name, signature, and date of |
and date |
signature |
PT name, signature, and date |
Indicate the physical therapist’s name, signature, and date of |
|
signature |
OT name, signature, and date |
Indicate the occupational therapist’s name, signature, and date of |
|
signature |
F00009 |
Page 1 of 3 |
Effective Date_03172014/Revised Date_05202014 |
Field Description |
Guidelines |
SLP name, signature, and date |
Indicate the speech language pathologist’s name, signature, and |
|
date of signature |
Provider Information and Required Signature |
|
Field Description |
Guidelines |
Provider name |
Enter the provider’s name |
CSHCN TPI |
Enter the provider’s Texas provider identifier (TPI) |
NPI |
Enter the provider’s national provider identifier (NPI) |
Taxonomy code |
Enter the provider’s taxonomy code |
Benefit code |
Enter CSN |
Provider contact name |
Enter the provider’s contact name |
Telephone number |
Enter the provider’s telephone number |
Fax number |
Enter the provider’s fax number |
Address/City/ZIP |
Enter the provider’s address, city, and ZIP |
Provider signature |
Provider must sign in this field |
Date |
Enter the date the form is signed |
Additional Requirements
•The GP or the GO modifier is required when requesting authorization for PT and OT services. PT should be requested using the GP modifier and OT should be requested using the GO modifier
•SLP services should be requested using the GN modifier
F00009 |
Page 2 of 3 |
Effective Date_03172014/Revised Date_05202014 |
CSHCN Services Program Authorization Request for Initial Outpatient Therapy (TP1)
Please print or type requested information below.
Client Information
First name: |
|
Last name: |
|
||
|
|
|
|
|
|
CSHCN Services Program number: 9- |
|
|
Date of birth: |
||
|
|
|
|
|
|
Address/City/ZIP: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnoses: |
|
|
|
|
|
|
|
|
|
|
|
Evaluation Summary: |
|
|
|
|
|
Date of evaluation: |
|
(A copy of the initial evaluation must be attached.) |
|||
|
|
||||
Type of evaluation: □ Physical Therapy (PT) |
□ Occupational Therapy (OT) □ Speech Language Pathology (SLP) |
||||
Comments:
Service Request:
Indicate procedure code(s), modifier, the dates of service, and the frequency per week or month. Dates of service cannot exceed six months. If possible, end requested date(s) of service on the last day of a month.
Procedure Code |
Modifier |
From Date |
To Date |
Frequency/Week |
Frequency/Month |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician name: |
Physician signature: |
Date: |
|
|
|
PT name: |
PT signature: |
Date: |
|
|
|
OT name: |
OT signature: |
Date: |
|
|
|
SLP name: |
SLP signature: |
Date: |
Provider Information and Required Signature:
Provider name:
CSHCN TPI: |
NPI: |
|
|
|
|
Taxonomy code: |
Benefit code: CSN |
|
|
|
|
Provider contact name: |
|
|
|
|
|
Telephone number: |
Fax number: |
|
|
|
|
Address/City/ZIP: |
|
|
|
|
|
|
|
|
Signature of provider: |
|
Date: |
|
|
|
F00009 |
Page 3 of 3 |
Effective Date_03172014/Revised Date_05202014 |