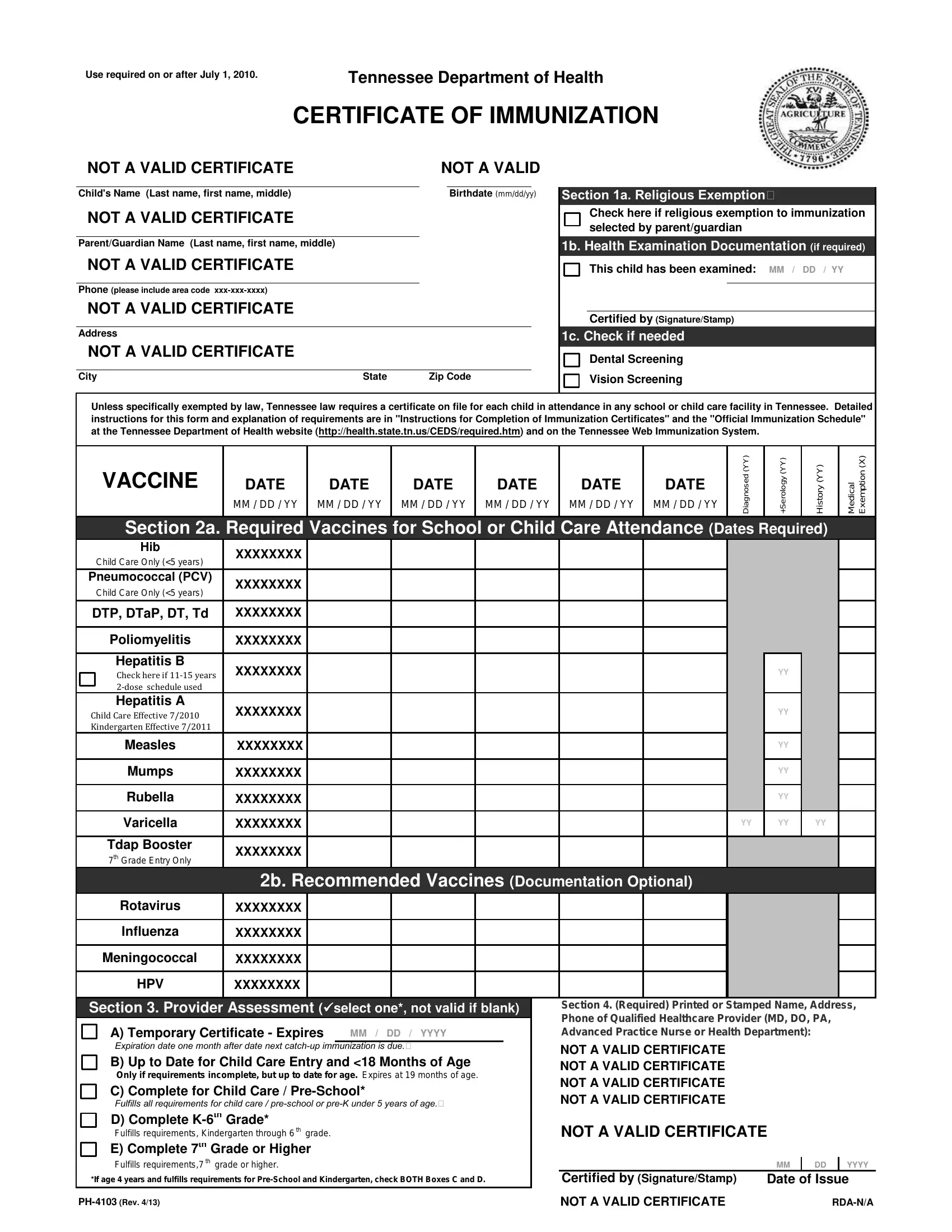
In states across the U.S., including Tennessee, the management of immunization records is a critical aspect of ensuring the health and safety of school-aged children. The Tennessee Immunization Form, mandated for use on or after July 1, 2010, by the Tennessee Department of Health, plays a vital role in this process. This document, officially known as the Certificate of Immunization, serves multiple purposes: it verifies a child's compliance with required vaccinations for school or child care attendance, provides options for religious exemptions, and outlines the health checks needed before entry into the educational system. It's structured to record a comprehensive list of vaccinations, including doses of DTaP, Polio, Hepatitis B, and MMR, among others. Additionally, the form addresses the need for health examinations, such as dental and vision screenings, and includes sections for documenting any medical or temporary immunization exemptions. Aimed at students entering childcare, pre-school, and grades up to high school, the Tennessee Immunization Form is an essential tool for parents, healthcare providers, and educational institutions to keep track of immunization status, ensuring a safer environment for all children.
| Question | Answer |
|---|---|
| Form Name | Tn Immunization Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | tennessee department of health certificate of immunization, covid vaccine card template tennessee, tn certificate of immunization, tennessee certificate of immunization form |
Use required on or after July 1, 2010. |
Tennessee Department of Health |
|
CERTIFICATE OF IMMUNIZATION
NOT A VALID CERTIFICATE |
|
NOT A VALID |
|||
|
|
|
|
|
|
Child's Name (Last name, first name, middle) |
|
|
Birthdate (mm/dd/yy) |
||
NOT A VALID CERTIFICATE |
|
|
|
|
|
|
|
|
|
|
|
Parent/Guardian Name (Last name, first name, middle) |
|
|
|
|
|
NOT A VALID CERTIFICATE |
|
|
|
|
|
|
|
|
|
|
|
Phone (please include area code |
|
|
|
|
|
NOT A VALID CERTIFICATE |
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
NOT A VALID CERTIFICATE |
|
|
|
|
|
|
|
|
|
||
City |
State |
Zip Code |
|||
Section 1a. Religious Exemption
Check here if religious exemption to immunization selected by parent/guardian
1b. Health Examination Documentation (if required)
This child has been examined: MM / DD / YY
Certified by (Signature/Stamp)
1c. Check if needed
Dental Screening
Vision Screening
Unless specifically exempted by law, Tennessee law requires a certificate on file for each child in attendance in any school or child care facility in Tennessee. Detailed instructions for this form and explanation of requirements are in "Instructions for Completion of Immunization Certificates" and the "Official Immunization Schedule" at the Tennessee Department of Health website (http://health.state.tn.us/CEDS/required.htm) and on the Tennessee Web Immunization System.
VACCINE
DATE |
DATE |
DATE |
DATE |
DATE |
DATE |
MM / DD / YY |
MM / DD / YY |
MM / DD / YY |
MM / DD / YY |
MM / DD / YY |
MM / DD / YY |
|
|
|
|
|
|
Diagnosed (YY)
+Serology (YY)
History (YY)
Medical Exemption (X)
Section 2a. Required Vaccines for School or Child Care Attendance (Dates Required)
Hib |
XXXXXXXX |
|
|
|
|
|
Child Care Only (<5 years) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pneumococcal (PCV) |
XXXXXXXX |
|
|
|
|
|
Child Care Only (<5 years) |
|
|
|
|
|
|
|
|
|
|
|
|
|
DTP, DTaP, DT, Td |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
Poliomyelitis |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B |
XXXXXXXX |
|
|
|
|
|
Check here if |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis A |
XXXXXXXX |
|
|
|
|
|
Child Care Effective 7/2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Kindergarten Effective 7/2011 |
|
|
|
|
|
|
Measles |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
Mumps |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
Rubella |
XXXXXXXX |
|
|
|
|
|
Varicella |
XXXXXXXX |
|
|
|
|
|
Tdap Booster |
XXXXXXXX |
|
|
|
|
|
7th Grade Entry Only |
|
|
|
|
|
|
|
|
|
|
|
|
|
YY |
|
|
|
|
|
YY |
|
|
|
|
|
YY |
|
|
|
|
|
YY |
|
|
|
|
|
YY |
|
|
|
|
YY |
YY |
YY |
|
|
|
|
2b. Recommended Vaccines (Documentation Optional) |
|||||||
Rotavirus |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Influenza |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Meningococcal |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HPV |
XXXXXXXX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Section 3. Provider Assessment (select one*, not valid if blank)
A) Temporary Certificate - Expires |
MM / DD / YYYY |
Expiration date one month after date next
B) Up to Date for Child Care Entry and <18 Months of Age
Only if requirements incomplete, but up to date for age. Expires at 19 months of age.
C) Complete for Child Care /
Fulfills all requirements for child care /
D) Complete
Fulfills requirements, Kindergarten through 6 th grade.
E) Complete 7th Grade or Higher
Fulfills requirements,7 th grade or higher.
*If age 4 years and fulfills requirements for
Section 4. (Required) Printed or Stamped Name, Address, Phone of Qualified Healthcare Provider (MD, DO, PA, Advanced Practice Nurse or Health Department):
NOT A VALID CERTIFICATE
NOT A VALID CERTIFICATE
NOT A VALID CERTIFICATE
NOT A VALID CERTIFICATE
NOT A VALID CERTIFICATE
|
MM |
DD |
YYYY |
Certified by (Signature/Stamp) |
Date of Issue |
||
NOT A VALID CERTIFICATE |
Vaccine Requirements for Attending Child Care Facilities,
Recommended Schedule of Required Doses for Attendance in Child Care /
For Children Who Started Immunizations Before Age 7 Years**
Required Vaccines with |
2 |
4 |
6 |
Total Doses Required*** For Assessment |
|||||
Months |
Months |
Months |
Month of |
Month |
(School |
of Complete For School Attendance on |
|||
footnote numbers in [ ] |
|||||||||
of Age |
of Age |
of Age |
Age |
of Age |
Entry) |
Immunization Certificate |
|||
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
[1] |
Hib HbOC or |
1 |
2 |
3 |
4 |
|
|
N/A for school (See Footnote [1]) |
|
[1] |
Hib |
1 |
2 |
3 |
4 |
|
|
N/A for school (See Footnote [1]) |
|
[1] |
Hib |
1 |
2 |
|
3 |
|
|
N/A for school (See Footnote [1]) |
|
[2] |
PCV |
1 |
2 |
3 |
4 |
|
|
N/A for school (See Footnote [2]) |
|
[3] |
DTP, DTaP, DT |
1 |
2 |
3 |
4 |
|
5 |
5 or 4 (See Footnote [3]) |
|
[4] |
Polio |
1 |
2 |
|
3 |
|
4 |
5, 4 or 3 (See Footnote [4]) |
|
[5] |
Hepatitis B |
1 |
2 |
|
3 |
|
|
3 (See Footnote [5]) |
|
[6] |
Hepatitis A |
|
|
|
1 |
|
2 |
2 (See Footnote [6]) |
|
[7] |
MMR |
|
|
|
1 |
|
2 |
2 (See Footnote [7]) |
|
[8] |
Varicella |
|
|
|
1 |
|
2 |
2 (See Footnote [8]) |
|
[9] |
Tdap |
|
|
|
|
|
|
1 (7th grade only) |
|
*These requirements were established in accordance with the current Recommended Childhood and
For children starting immunizations at age 7 years or older, refer to the catch up schedule available at the Department of Health website or the ACIP
***Children who are behind schedule may attend while in the process of completing the requirements with minimum intervals as indicated below.
Minimum Ages For Initial Immunization And Minimum Intervals Between Doses
|
Vaccine |
Minimum Age For |
Minimum interval |
Minimum interval |
Minimum interval |
Minimum interval |
With respect to the intervals, 1 month is a minimum of 4 weeks or 28 days. |
|
First Dose |
from dose 1 to 2 |
from dose 2 to 3 |
from dose 3 to 4 |
from dose 4 to 5 |
||
|
|
|
|||||
[1] |
Hib (Primary Series) |
|
|
|
|
|
|
|
HbOC & |
6 weeks |
1 month |
1 month |
See Footnote [1] |
N/A |
Do not restart any series, no matter how long since the previous dose. Doses |
|
6 weeks |
1 month |
See Footnote [1] |
N/A |
N/A |
given ≤ 4 days before the minimum age or the minimum interval may be counted |
|
[2] |
PCV |
6 weeks |
1 month |
1 month |
See Footnote [2] |
N/A |
as valid. |
[3] |
DTP/DTaP (DT) |
6 weeks |
1 month |
1 month |
6 months |
See Footnote [3] |
Two different live vaccines must be given on the same day or spaced at least 28 |
[4] |
Polio |
6 weeks |
1 month |
1 month |
See Footnote [4] |
See Footnote [4] |
days apart. |
[5] |
Hepatitis B |
birth |
1 month |
See Footnote [5] |
N/A |
N/A |
|
[6] |
Hepatitis A |
12 months |
6 months |
|
|
|
|
[7] |
MMR |
12 months |
1 month |
N/A |
N/A |
N/A |
|
[8] |
Varicella |
12 months |
3 months [8] |
N/A |
N/A |
N/A |
|
[9] |
Tdap |
See Footnote [9] |
|
|
|
|
|
Footnotes
[1]The number of doses of Hib depends on age at 1st dose and brand of vaccine given. The last dose in the series necessary to meet requirements, whether 3rd or 4th, should be given at least 2 months after the previous dose and not before 12 months of age. One dose is sufficient to meet requirements if it is given at age 15 months or later. Hib is required for children younger than 5 years attending child care facilities. Hib is not required for kindergarten or higher grades and is not indicated for children who have reached the 5th birthday. If given on schedule,
[2]The number of doses in the PCV series depends on age at 1st dose. The last dose in the series should be given at least 2 months after the previous dose and not before 12 months of age. One dose of PCV is required for all children aged
[3]The minimum interval between the 4th and 5th doses is 6 months: dose 4 may be given as early as 12 months, but typically is given at age
4th dose was on or after the 4th birthday, the 5th dose is not needed. The 4th dose should be administered a minimum of 6 months after the 3rd dose. However, the 4th dose does not need to be repeated if administered ≥ 4 months after dose 3. Total doses of diphtheria and tetanus toxoids should not exceed 6 before the 7th birthday.
[4]The final dose of the polio vaccine series must be given on or after the 4th birthday and at least 6 months after the previous dose. If 4 doses are administered before the 4th birthday, a 5th dose should be given on or after the 4th birthday. If the 3rd dose of an all IPV or all OPV series is given on or after the 4th birthday and at least 6 months after the 2nd dose, a 4th dose is not needed.
[5]The 3rd valid dose of hepatitis B vaccine must be at least 4 months after dose 1 and 2 months after dose 2 and not before 24 weeks of age. If the 3rd dose given is not valid for all criteria, a 4th dose is necessary.
[6]One dose of hepatitis A vaccine is required for all children in child care aged 18 months or greater. The recommended schedule is for two doses, 6 to 18 months apart, beginning at one year of age. Proof of two doses, at least 6 months apart, is required for Kindergarten entry. Hepatitis A vaccine is not required for entry in older school grades.
[7]The MMR requirement is 2 doses of measles vaccine, 2 doses of mumps vaccine and 2 doses of rubella vaccine, in combination or separately. Dose 2 of MMR is routinely given at
[8]The varicella requirement is for 2 doses of varicella vaccine or history of disease for all students entering K or 7th grade, and new entrants into a Tennessee school in any other grade. The second dose is recommended 3 or more months after the first dose, routinely at age
[9]A single dose of Tdap is required for 7th grade entry. Tdap meets the requirement if given any time after the 7th birthday. If Tdap is needed, it may be given regardless of interval since last Td.
Use Required on or After July 1, 2010 |