
Using PDF forms online can be very simple with our PDF editor. You can fill in transfer information sheet navy here painlessly. To keep our editor on the forefront of convenience, we work to put into operation user-oriented capabilities and improvements on a regular basis. We are routinely happy to receive suggestions - play a vital role in reshaping PDF editing. It just takes several basic steps:
Step 1: Click on the orange "Get Form" button above. It will open up our pdf editor so you can begin filling out your form.
Step 2: With our advanced PDF tool, it is possible to do more than just fill out blank form fields. Try each of the features and make your docs appear professional with customized textual content put in, or tweak the original input to perfection - all that comes with the capability to incorporate any images and sign the document off.
This PDF form will require specific info to be typed in, therefore be sure you take your time to type in what is expected:
1. Whenever completing the transfer information sheet navy, be certain to incorporate all of the needed blank fields in their associated section. It will help to expedite the process, making it possible for your information to be handled quickly and appropriately.
2. Now that the previous part is finished, you're ready put in the necessary details in Name and Relationship Address, Advance Pay Desired Yes Complete, Advance DLA Desired Yes No married, Will your dependents accompany you, Are you using your COT entitlement, Home of Record CITY STATE, Will TLA Claim be submitted Yes No, Date, B DIVISION OFFICER complete, Indicate Members Transfer Date if, Inform individual that transfer, Transfer Information Sheet and, Copy of PCS Orders Request for, and Application For Transportation of so you're able to progress to the 3rd step.
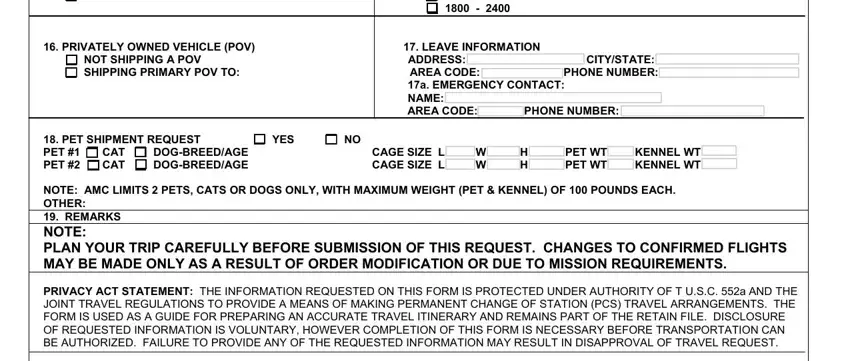
3. This next part will be hassle-free - fill out all of the fields in Application For Transportation of, Required obligated service has, Transfer Evaluation E and, CPCLeading Yeoman informed to make, Inform member to pick up Medical, I certify that I have taken or, C APPROVING AUTHORITY FOR COMMAND, I certify that I have reviewed the, PRIVACY ACT STATEMENT, Date, Date, and The information requested on this to finish this part.
4. Filling in PASSENGER RESERVATION REQUEST PCS, INITIAL, CHANGE, THIS FORM MUST BE TYPED, MEMBERS NAME LAST FIRST MI NAME, RANKRATE AGENDER, SSN A DOB, COMMAND DETACH DATE, MEMBERS LOCAL PHONE EMAIL, MEMBERS TRAVEL INCLUDING LEAVE, TRAVELING WITH SPONSOR OR, and TYPE SEAT REQUESTED FLIGHT TIME is paramount in the next step - be certain to be patient and take a close look at each and every field!
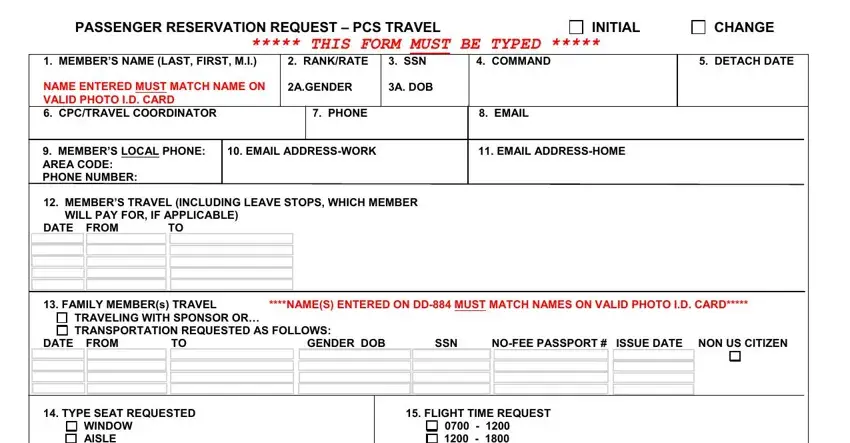
As to COMMAND DETACH DATE and RANKRATE AGENDER, ensure that you review things in this section. The two of these are thought to be the most significant fields in this PDF.
5. And finally, this last portion is precisely what you will have to finish before finalizing the document. The blanks at issue include the next: YES, CAT CAT, DOGBREEDAGE CAGE SIZE L W H PET WT, NOT SHIPPING A POV ADDRESS, and TYPE SEAT REQUESTED FLIGHT TIME.
Step 3: Right after looking through the filled in blanks, hit "Done" and you're done and dusted! After creating a7-day free trial account at FormsPal, it will be possible to download transfer information sheet navy or send it via email without delay. The PDF document will also be accessible through your personal account menu with all of your adjustments. With FormsPal, it is simple to fill out documents without having to worry about personal data breaches or entries being distributed. Our secure platform ensures that your personal details are stored safe.