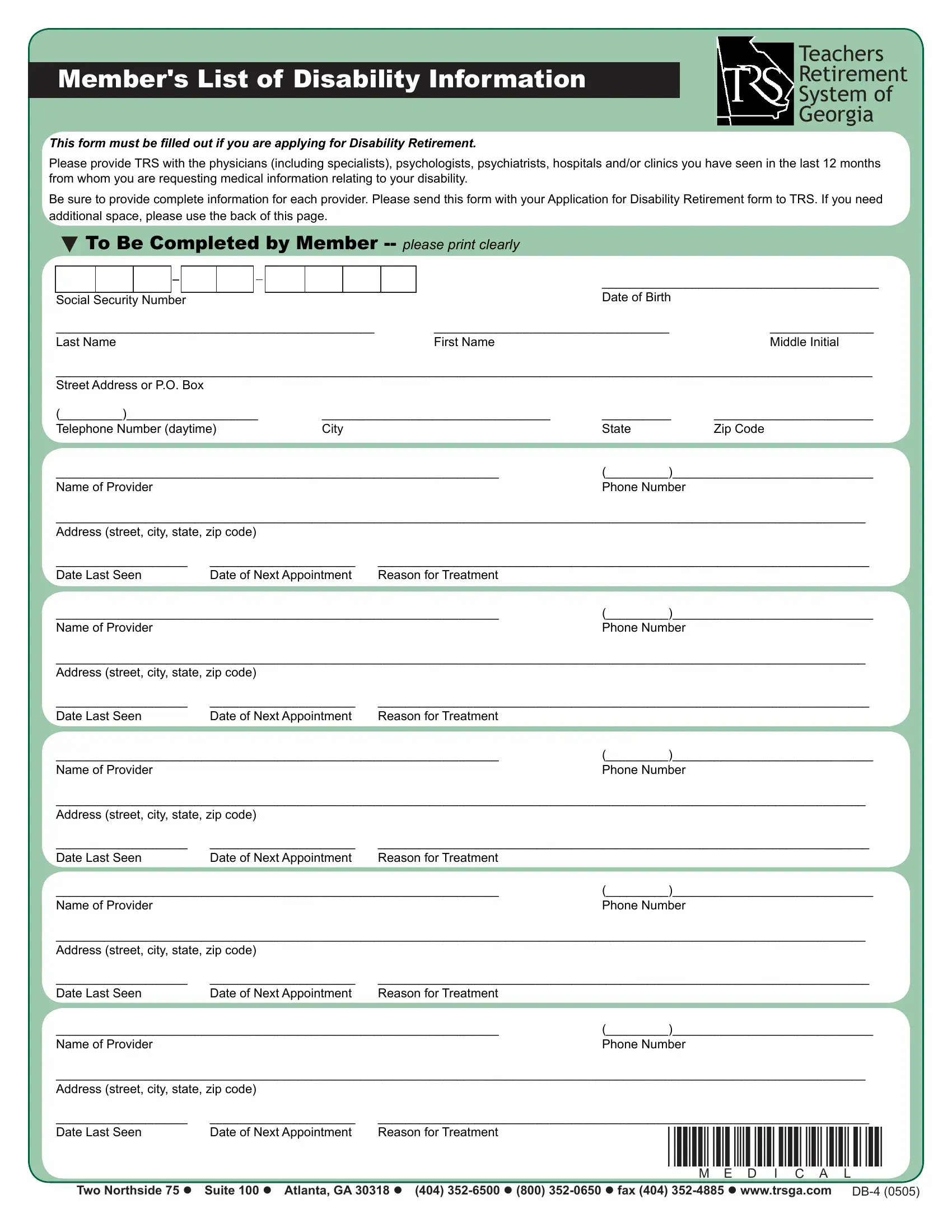
When educators in Georgia face the unfortunate event of a disability, the Teachers Retirement System of Georgia (TRS) necessitates the completion of the TRS DB-4 form, a pivotal document in applying for disability retirement. This form meticulously collects information on the medical professionals, including specialists such as psychologists and psychiatrists, as well as hospitals and clinics that the member has consulted within the past year for conditions related to their disability. It is crucial for members to fill out this form with comprehensive details for each medical provider, from names and phone numbers to addresses and the dates of appointments. This documentation plays an essential role in the evaluation process of the disability retirement application, ensuring that TRS has all the necessary medical information to assess the member's retirement claim accurately. Therefore, it is imperative for members to include this form alongside their Application for Disability Retirement form and to utilize the additional space at the back of the page if needed. The submission of this thoroughly completed form to TRS is a critical step in the journey toward securing disability retirement for educators who have dedicated their careers to the education system in Georgia.
| Question | Answer |
|---|---|
| Form Name | Trs Form Db 4 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | physicians, Georgia, print disability forms texas, trs disability retirement texas |
Member's List of Disability Information
This form must be illed out if you are applying for Disability Retirement.
Teachers
Retirement
System of
Georgia
Please provide TRS with the physicians (including specialists), psychologists, psychiatrists, hospitals and/or clinics you have seen in the last 12 months from whom you are requesting medical information relating to your disability.
Be sure to provide complete information for each provider. Please send this form with your Application for Disability Retirement form to TRS. If you need additional space, please use the back of this page.
To Be Completed by Member
|
|
|
|
|
|
|
|
|
|
|
|
________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth |
|
Social Security Number |
|
||||||||||||
______________________________________________ |
|
__________________________________ |
_______________ |
||||||||||
Last Name |
First Name |
Middle Initial |
|||||||||||
______________________________________________________________________________________________________________________
Street Address or P.O. Box
(_________)___________________ |
_________________________________ |
__________ |
_______________________ |
Telephone Number (daytime) |
City |
State |
Zip Code |
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
Phone Number |
|
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
*MEDICAL* |
|
|||
Two Northside 75 Suite 100 Atlanta, GA 30318 (404)