The Texas Vaccines for Children Program (TVFC), through its detailed Provider Enrollment and Profile forms, plays a crucial role in ensuring the health and well-being of Texas' younger population by facilitating access to essential vaccinations at no cost to eligible children. Designed meticulously to cater to various health care settings, the enrollment form requires comprehensive details about the medical facility, the provider’s qualifications, and a commitment to adhere to the program's guidelines, such as screening patients for eligibility, maintaining accurate records for a minimum of three years, and complying with designated vaccination schedules. Moreover, it lays down clear expectations regarding the administration of vaccines—highlighting that vaccines provided by the Department of State Health Services (DSHS) cannot be charged for, while setting a limit on administration fees that can be charged to non-Medicaid eligible patients. The form further mandates that providers cannot deny vaccination based on the guardian's inability to pay an administrative fee, ensuring that financial constraints do not prevent eligible children from receiving vital immunizations. Additionally, the Provider Profile sections gather statistical data on the anticipated vaccination needs, thereby enabling better planning and resource allocation. This careful orchestration of requirements underscores a strong commitment to public health, aiming to reduce vaccine-preventable diseases among children, regardless of their financial circumstances.
| Question | Answer |
|---|---|
| Form Name | Tvfc Form E6 102 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | 2019 tvfc re enrollment, underinsured, TEXAS, 2007 |
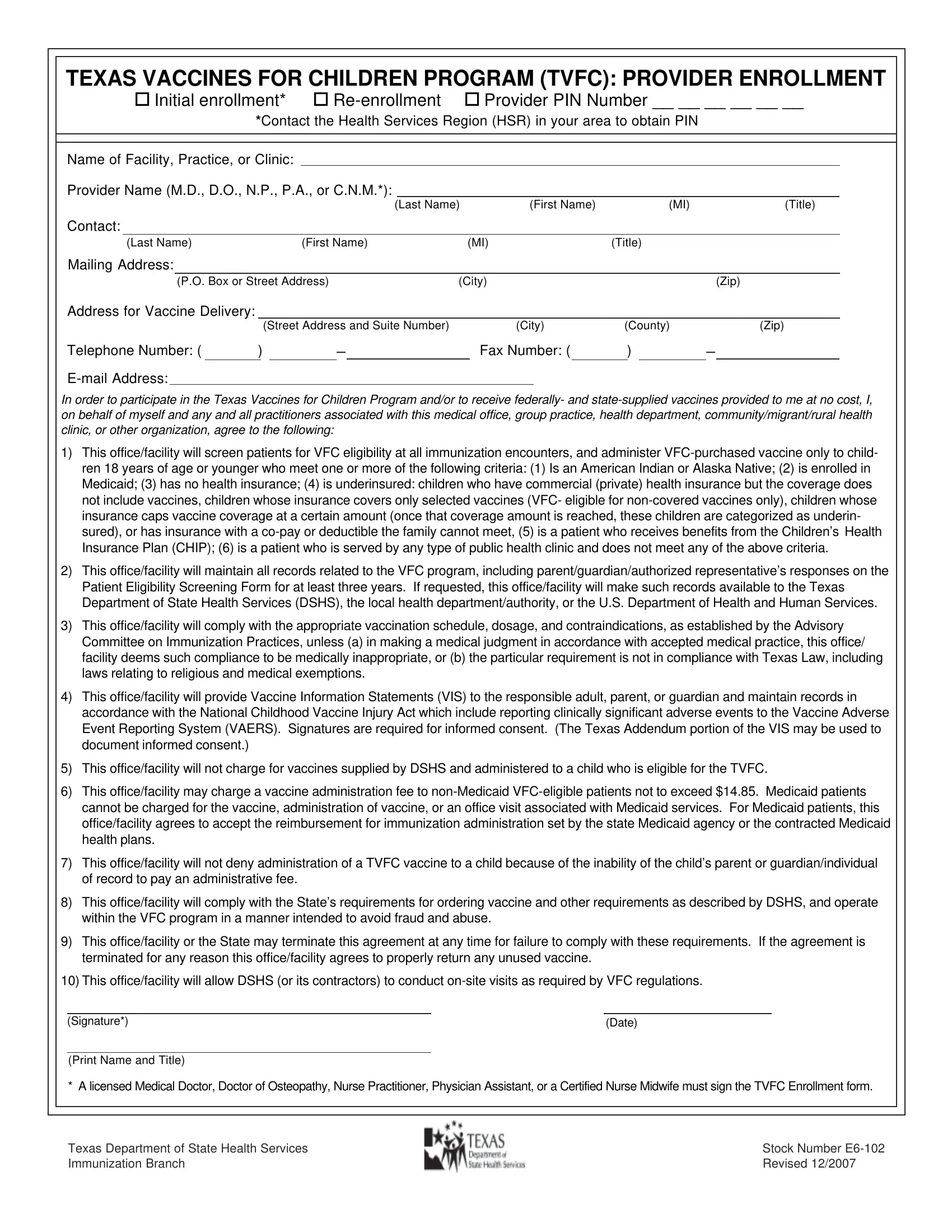
TEXAS VACCINES FOR CHILDREN PROGRAM (TVFC): PROVIDER ENROLLMENT
! Initial enrollment* !
*Contact the Health Services Region (HSR) in your area to obtain PIN
Name of Facility, Practice, or Clinic:
Provider Name (M.D., D.O., N.P., P.A., or C.N.M.*):
(Last Name)(First Name)(MI)(Title)
Contact:
(Last Name)(First Name)(MI)(Title)
Mailing Address:
(P.O. Box or Street Address)(City)(Zip)
Address for Vaccine Delivery:
|
|
|
(Street Address and Suite Number) |
(City) |
(County) |
|
(Zip) |
||||||
Telephone Number: ( |
) |
|
|
|
Fax Number: ( |
) |
|
|
|
||||
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In order to participate in the Texas Vaccines for Children Program and/or to receive federally- and
1)This office/facility will screen patients for VFC eligibility at all immunization encounters, and administer
2)This office/facility will maintain all records related to the VFC program, including parent/guardian/authorized representative’s responses on the Patient Eligibility Screening Form for at least three years. If requested, this office/facility will make such records available to the Texas Department of State Health Services (DSHS), the local health department/authority, or the U.S. Department of Health and Human Services.
3)This office/facility will comply with the appropriate vaccination schedule, dosage, and contraindications, as established by the Advisory Committee on Immunization Practices, unless (a) in making a medical judgment in accordance with accepted medical practice, this office/ facility deems such compliance to be medically inappropriate, or (b) the particular requirement is not in compliance with Texas Law, including laws relating to religious and medical exemptions.
4)This office/facility will provide Vaccine Information Statements (VIS) to the responsible adult, parent, or guardian and maintain records in accordance with the National Childhood Vaccine Injury Act which include reporting clinically significant adverse events to the Vaccine Adverse Event Reporting System (VAERS). Signatures are required for informed consent. (The Texas Addendum portion of the VIS may be used to document informed consent.)
5)This office/facility will not charge for vaccines supplied by DSHS and administered to a child who is eligible for the TVFC.
6)This office/facility may charge a vaccine administration fee to
7)This office/facility will not deny administration of a TVFC vaccine to a child because of the inability of the child’s parent or guardian/individual of record to pay an administrative fee.
8)This office/facility will comply with the State’s requirements for ordering vaccine and other requirements as described by DSHS, and operate within the VFC program in a manner intended to avoid fraud and abuse.
9)This office/facility or the State may terminate this agreement at any time for failure to comply with these requirements. If the agreement is terminated for any reason this office/facility agrees to properly return any unused vaccine.
10)This office/facility will allow DSHS (or its contractors) to conduct
(Signature*) |
(Date) |
(Print Name and Title)
* A licensed Medical Doctor, Doctor of Osteopathy, Nurse Practitioner, Physician Assistant, or a Certified Nurse Midwife must sign the TVFC Enrollment form.
Texas Department of State Health Services |
Stock Number |
Immunization Branch |
Revised 12/2007 |
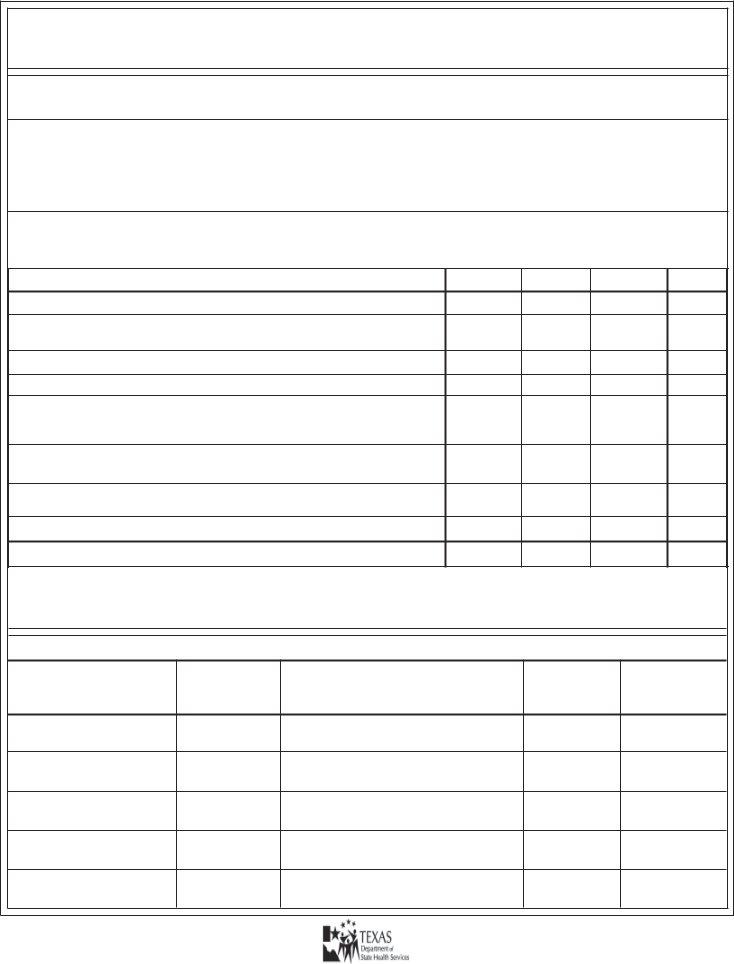
TEXAS VACCINES FOR CHILDREN PROGRAM
PROVIDER PROFILE FOR PIN ___ ___ ___ ___ ___ ___
Is your facility a Federally Qualified Health Center, Migrant Health Clinic, or Rural Health Clinic?
(Circle one) YES |
NO |
Type of Clinic: ( √ check one) |
|
! Public Health Department/District |
! |
! Public Hospital |
! |
! Other Public Clinic |
! |
Private Hospital
Private Practice (Individual or Group)
Other Private Clinic
PATIENT PROFILE:
Please enter the number of children for each of the following categories and by
age group who will be vaccinated at your clinic in the next
NUMBER OF CHILDREN IN EACH CATEGORY |
< 1 year old 1 - 6 years 7 - 18 years Total |
Enrolled in Medicaid.
Uninsured. (Note: Children enrolled in Health Maintenance Organizations are considered insured)
American Indians.
Alaskan Natives.
Underinsured. (Has health insurance that Does Not pay for vaccines, has a
(For Public Health Clinic Use ONLY) Children who do not meet any of the above criteria, but still receive vaccinations at public health clinics.
Children who receive benefits from the Children’s Health Insurance Plan (CHIP).
Children who are vaccinated in your practice, but are NOT
TOTAL PATIENTS: (Add columns)
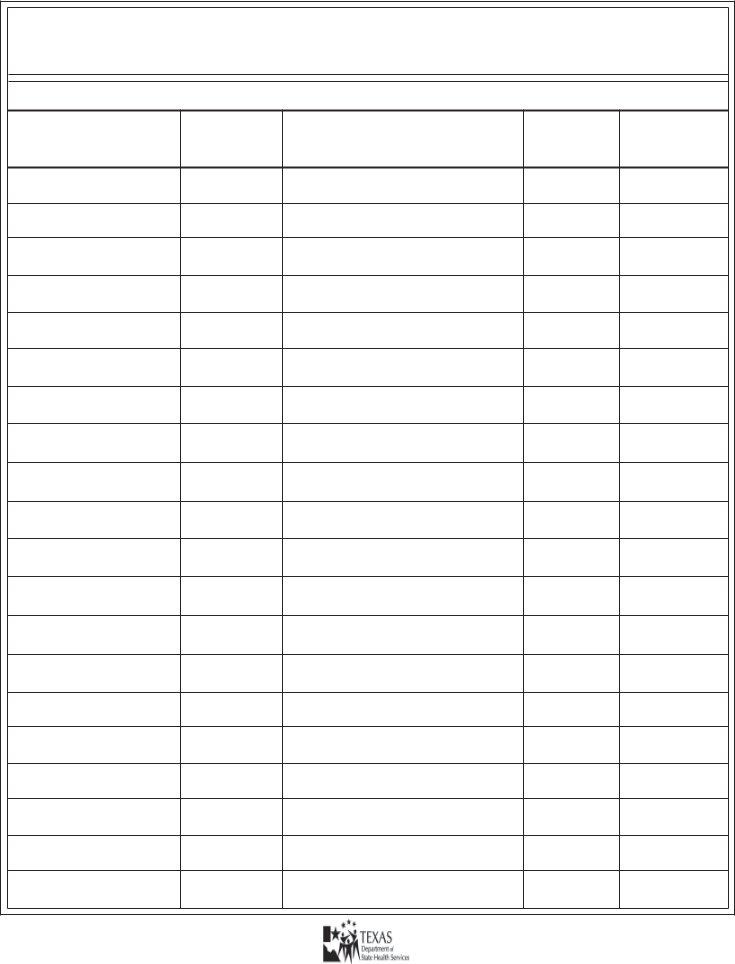
TEXAS VACCINES FOR CHILDREN PROGRAM PROVIDER LIST
Please list all individuals within the practice who will be administering TVFC supplied vaccine.
Last Name
(List provider who signed Provider Enrollment Formfirst)
First Name
Middle |
Title (M.D., D.O., |
National |
Initial |
N.P., P.A., R.N., |
Provider |
|
L.V.N., M.A.) |
Identification |
|
|
|
Medical
License
Number
Specialty
(Family Medicine, Pediatrics, etc.)
Texas Department of State Health Services |
Stock Number |
Immunization Branch |
Revised 12/2007 |
TEXAS VACCINES FOR CHILDREN PROGRAM
PROVIDER
Please list all individuals within the practice who will be administering TVFC supplied vaccine.
Last Name
(List provider who signed Provider Enrollment Form first)
First Name
Middle |
Title (M.D., |
National |
Initial |
D.O., N.P., P.A., |
Provider |
|
R.N., L.V.N., M.A.) |
Identification |
|
|
|
Medical
License
Number
Specialty
(Family Medicine, Pediatrics, etc.)
Texas Department of State Health Services |
Stock Number |
Immunization Branch |
Revised 12/2007 |