In the landscape of clinical tools designed to assess neurological conditions, the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) stands out for its specific focus on spasmodic torticollis, also known as cervical dystonia. This condition, characterized by involuntary muscle contractions in the neck, can significantly impact a patient's quality of life. Developed with the support of WE MOVE and partially funded by an educational grant from Allergan, TWSTRS provides a structured method for clinicians to document the severity of torticollis, the disability it imposes, and the associated pain. The scale is comprehensive, featuring a maximum severity score of 35 across various categories such as maximal excursion, sensory tricks, and shoulder elevation, as well as a disability scale and a pain scale. Alongside the examination form, the packet includes 50 tear-off copies for practical use and a laminated card for quick reference, underscoring its utility in both research and clinical settings. The inclusion of an injection record underlines its application in monitoring treatment effectiveness, specifically in cases where botulinum toxin injections are employed. This meticulous approach to quantifying the impacts of cervical dystonia underscores the TWSTRS's vital role in enhancing patient care and facilitating ongoing research.
| Question | Answer |
|---|---|
| Form Name | Twstrs Rating Scale Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | twstrs, toronto western spasmodic torticollis rating scale pdf, toronto western spasmodic torticollis rating scale, 2002 |
Toronto Western
Spasmodic Torticollisll
Rating Scalele (TWSTRS)11
WE MOVE is pleased to provide this clinical tool for assessing and documenting the status of patients with spasmodic torticollisÑalso known as cervical dystonia. Additional scales and assessment forms are available at
www.wemove.org
This packet contains
¥50
¥A
¥
Presented by WE MOVE
PHONE:
Production funded in part by an unrestricted educational grant from Allergan.
WE MOVE makes every effort to ensure the accuracy of this publication. Since there are daily advances in medical science, WE MOVE invites you to visit the Web site at www.wemove.org for view the most recent version of this document.
Toronto Western
Spasmodic
Torticollis
Rating Scale
(TWSTRS)11
PRESENTED BY WE MOVEª | © 2002
I. Torticollis Severity Scale (MAXIMUM = 35)
A. Maximal Excursion
1.Rotation (turn: right or left) 0 = None [0¡]
1 = Slight [< 1/4 range, 1¡Ð 22¡]
2 = Mild [1/4 Ð 1/2 range, 23¡Ð 45¡]
3 = Moderate [1/2 Ð 3/4 range, 46¡Ð 67¡] 4 = Severe [> 3/4 range, 68¡Ð90¡]
2.Laterocollis (tilt: right or left, exclude shoulder elevation) 0 = None [0¡]
1 = Mild [1¡Ð15¡]
2 = Moderate [16¡Ð35¡]
©WE MOVEª 2002
1. Consky ES, Lang AE. Clinical assessments of patients with cervical dystonia. In: Jankovic J, Hallett M, eds. Therapy with Botulinum Toxin. New York, NY: Marcel Dekker,

TWSTRS Examination Record [to be completed by the examiner] |
||||
Patient |
|
|
Chart No. |
|
Date |
| |
| |
Time |
AM PM |
MONTH |
|
DAY |
YEAR |
©WE MOVEª 2002 |
I. Torticollis Severity Scale (MAXIMUM = 35)
Rate maximum amplitude of excursion asking patient not to oppose the abnormal movement; examiner may use |
S C O R E |
|
||||||
A. Maximal Excursion distracting or aggavating maneuvers. When degree of deviation is between scores, choose the higher of the two. |
|
|||||||
1. Rotation |
0 |
1 |
2 |
3 |
4 |
|
|
|
|
|
|
|
|
|
|
|
|
2. Laterocollis |
0 |
1 |
2 |
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Anterocollis or Retrocollis |
|
|
|
|
|
|
|
|
a. Anterocollis |
0 |
1 |
2 |
3 |
|
|
|
|
b. Retrocollis |
0 |
1 |
2 |
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Lateral shift |
0 |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Sagittal shift |
0 |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. Duration Factor |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
(Weighted x 2) |
|
(X 2) |
(X 2) |
(X 2) |
(X 2) |
(X 2) |
|
|
|
|
|
|
|
|
|
|
|
C. Effect of Sensory Tricks |
0 |
1 |
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. Shoulder Elevation/Anterior Displacement |
0 |
1 |
2 |
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
E. Range of Motion |
0 |
1 |
2 |
3 |
4 |
|
|
|
|
|
|
|
|
|
|
|
|
F. Time |
0 |
1 |
2 |
3 |
4 |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
II. Disability Scale (MAXIMUM = 30) |
|
|
|
SUBTOTAL SEVERITY |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. Work |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
B. Activities of Daily Living |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
C. Driving |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
D. Reading |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
E. Television |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
F. Activities Outside the Home |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
|
|
SUBTOTAL DISABILITY |
|
|
||
III. Pain Scale (MAXIMUM = 20) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
A. Severity of Pain (worst + best + (2*usual))/4 |
Best ____ |
Worst ____ |
Usual ____ |
|
|
|||
|
|
|
|
|
|
|
|
|
B. Duration of Pain |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
C. Disability Due to Pain |
0 |
1 |
2 |
3 |
4 |
5 |
|
|
INJECTION RECORD ON REVERSE SIDE
SUBTOTAL PAIN
TOTAL TWSTRS SCORE
PHYSICIAN’S SIGNATURE
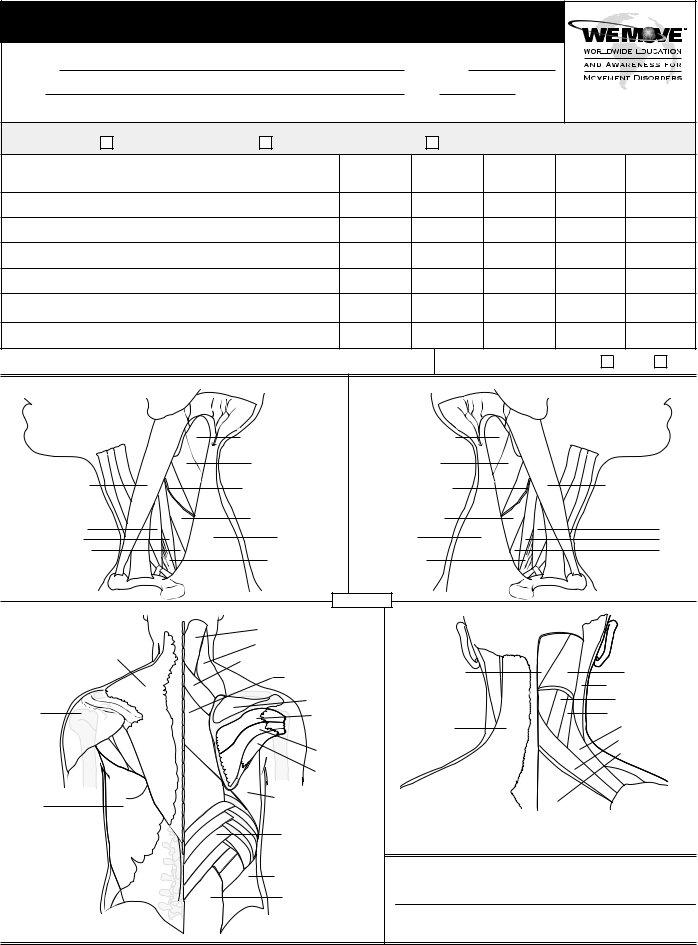
Injection Record [indicate injection sites on diagrams provided] |
|
|
|
||||
Patient |
|
|
|
Chart No. |
|
|
|
Date |
| |
|
| |
Time |
AM PM |
|
|
|
MONTH |
DAY |
YEAR |
|
|
©WE MOVEª 2002 |
|
|
|
|
|
|
|
||
Agent Injected: |
BOTOX _____ Units/ml. |
Dysport _____ Units/ml. |
MYOBLOC/Neurobloc _____ Units in _____ ml. |
||||
|
Muscle Injected |
|
Units |
Volume |
Number of |
Total |
Total |
|
|
Injected |
Injected |
Injections |
Units |
Volume |
|
|
|
|
|||||
Total Amount Administered _____________ Total Amount Used _____________
Electromyography Utilized?
Yes
No
|
Semispinalis capitis m. |
|
|
Splenius capitis m. |
|
Sternocleidomastoid m. |
Spinal accessory nerve |
|
|
||
Scalene muscles: |
Levator scapulae m. |
|
Anterior |
Trapezius m. |
|
Middle |
||
|
||
Posterior |
|
|
|
Brachial plexus |
Semispinalis capitis m. |
|
|
Splenius capitis m. |
|
|
Spinal accessory nerve |
Sternocleidomastoid m. |
|
|
||
Levator scapulae m. |
Scalene muscles: |
|
Trapezius m. |
Anterior |
|
Middle |
||
|
||
|
Posterior |
|
Brachial plexus |
|
m. = muscle
|
|
Splenius capitis m. |
|
|
Levator scapulae m. |
|
Trapezius m. |
Rhomboideus minor m. |
|
|
|
|
|
Rhomboideus major m. |
|
|
Supraspinatus m. |
Deltoid m. |
|
Infraspinatus m. |
|
|
|
|
|
Teres major m. |
|
|
Teres minor m. |
Latissimus |
|
Serratus anterior m. |
|
|
|
dorsi m. |
|
|
|
|
Serratus posterior |
|
|
inferior m. |
|
|
Oblique internus m. |
|
|
Erector spinae m. |
Semispinalis m. |
Splenius capitis m. |
|
Sternocleidomastoid m. |
|
Splenius cervicalis m. |
|
Longissimus capitis m. |
Trapezius m. |
Levator scapulae m. |
|
Rhomboid minor m. |
|
Rhomboid major m. |
PHYSICIAN’S SIGNATURE
Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS)