
This PDF editor was developed to be as easy as possible. As soon as you stick to these actions, the process of filling out the ub04 claim forms file is going to be easy.
Step 1: You can choose the orange "Get Form Now" button at the top of the following page.
Step 2: Now you can manage the ub04 claim forms. You need to use our multifunctional toolbar to include, erase, and alter the content material of the document.
Type in the essential material in each section to complete the PDF ub04 claim forms
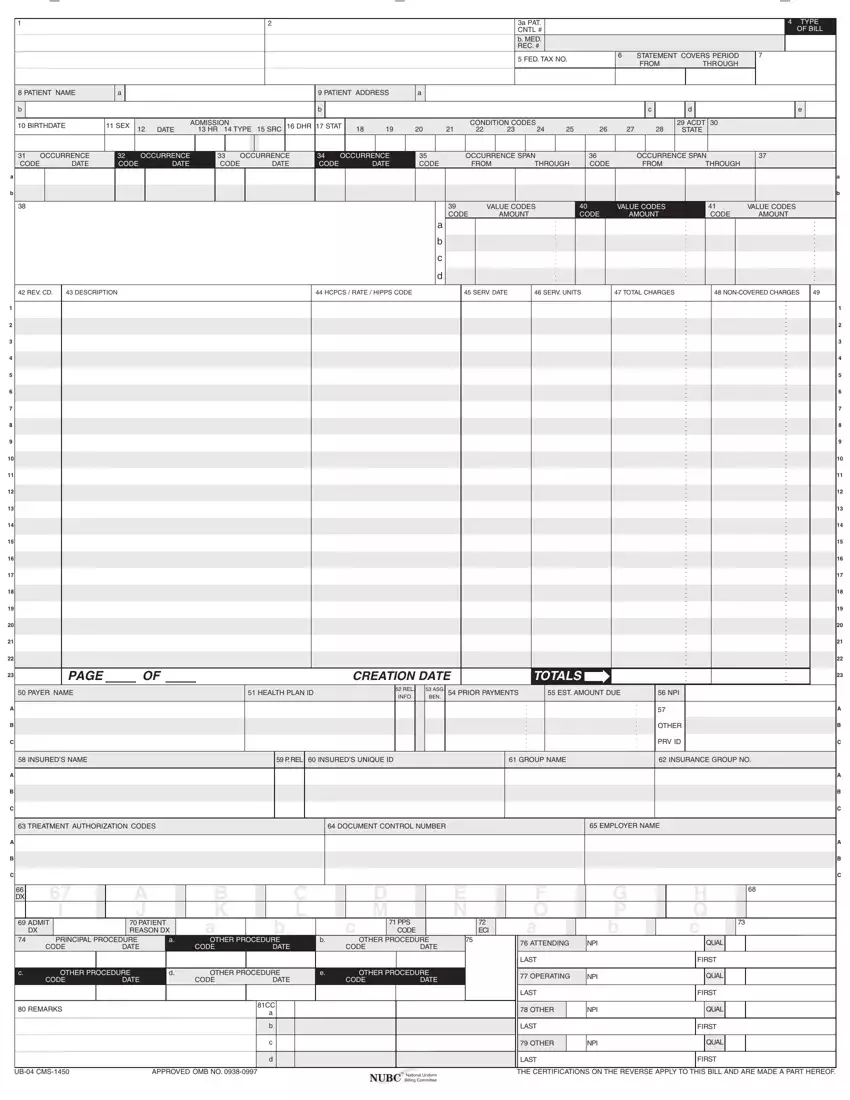
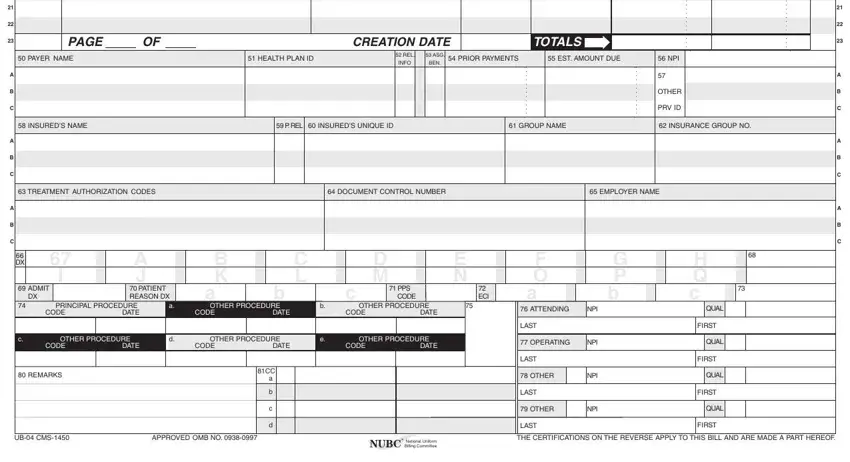
Provide the necessary information in the field PAGE, CREATION, DATE, TOTALS, PAYER NAME, HEALTH PLAN ID, REL INFO, ASG BEN, PRIOR PAYMENTS, EST AMOUNT DUE, NPI, OTHER, PRV ID, INSUREDS NAME, and P REL INSUREDS UNIQUE ID.
The system will ask for more details as a way to easily fill in the part SEE httpwwwnubcorg FOR MORE.
Step 3: Select "Done". You can now upload your PDF form.
Step 4: In order to avoid probable upcoming troubles, you should always obtain up to a few copies of every single form.
