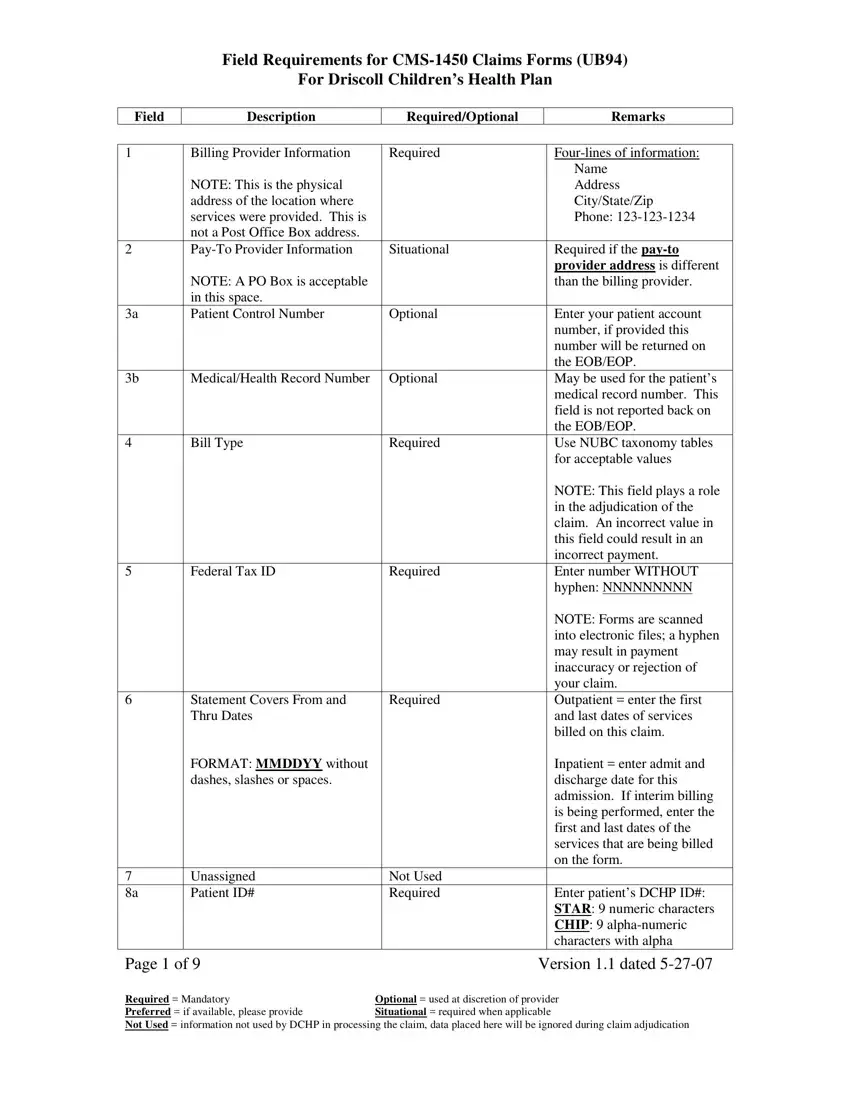
The UB-94 form, also recognized as the CMS-1450 claim form, stands as a critical document in the medical billing and insurance filing process. This form encompasses a range of fields tailored to capture exhaustive details about the medical services provided to patients, making it indispensable for clinicians, medical facilities, and billing professionals working within the realm of healthcare. Key sections of this form meticulously outline the requisite information for billing provider details, patient demographics, service dates, and charges, alongside specific healthcare services rendered. Requirements vary from mandatory ones, such as the billing provider's information and federal tax ID, to situational or optional fields like patient control numbers or various condition codes, underscoring the adaptability of the form based on the unique circumstances of each healthcare encounter. Precise details such as the patient’s name, address, state, date of birth, sex, and admission dates highlight the necessity of accuracy in completing the form. Additionally, the form delves into the intricacies of insurance billing, necessitating information on prior payments, payer names, and insurance IDs, thereby acting as a comprehensive tool to streamline the financial dimensions of patient care. Given its pivotal role in the adjudication of claims, an incorrect or incomplete UB-94 form can precipitate significant ramifications for payment accuracy, necessitating a keen understanding of its requirements and an attention to detail when populating its fields.
| Question | Answer |
|---|---|
| Form Name | Ub 94 Form |
| Form Length | 9 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 15 sec |
| Other names | ICD9, HCPCS, NPI, ub 94 |
