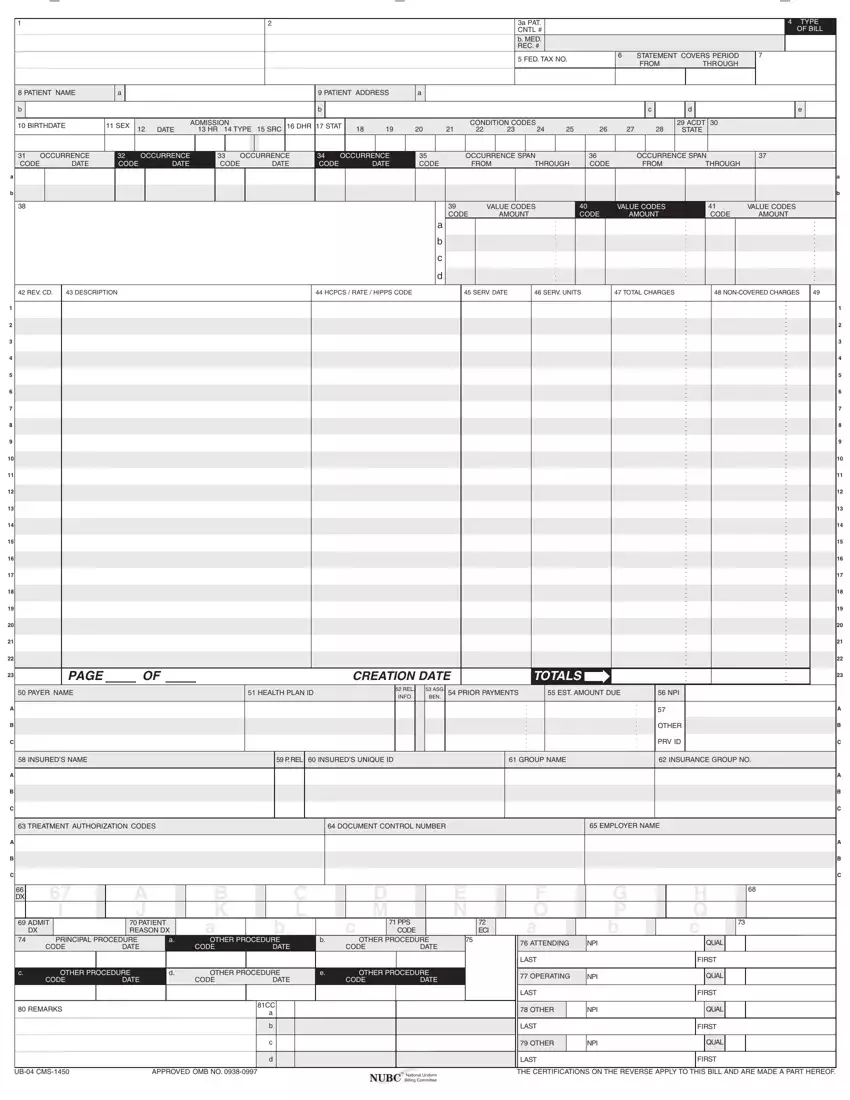
The UB-04 form, also recognized as the CMS-1450, is a crucial document extensively utilized within the healthcare sector, particularly by hospitals and other healthcare facilities to bill insurance companies for services rendered. This comprehensive form encapsulates a wealth of information, ranging from patient identification details like name and address, admission and discharge dates, to the intricacies of the medical services provided, including diagnosis codes, procedural codes, and the costs associated. Each section of the form, from fields 1-81, is meticulously designed to capture specific data, ensuring a standardized approach to submitting claims. Not only does this form serve as a bridge between healthcare providers and insurance entities, but it also adheres to strict compliance and ethical standards, as outlined by its accompanying legal notices and certifications. This ensures that all submitted claims are accurate, truthful, and in alignment with federal and state laws, thereby minimizing the risk of fraud and facilitating a smoother transaction process for both parties involved. Understanding the complexities and the importance of accurately completing the UB-04 form cannot be overstated, as it directly impacts the reimbursement process and ultimately the financial health of healthcare institutions.
| Question | Answer |
|---|---|
| Form Name | Ub04 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ub 04 form revenue codes, blank ub 04 form, ub04 form, ub 04 form |
