
With the help of the online tool for PDF editing by FormsPal, you'll be able to complete or alter ucla medical reports right here and now. To make our tool better and less complicated to work with, we consistently implement new features, with our users' feedback in mind. All it requires is a few simple steps:
Step 1: Simply click the "Get Form Button" above on this webpage to open our form editor. This way, you'll find all that is necessary to fill out your file.
Step 2: With the help of our online PDF tool, you may accomplish more than merely complete blank fields. Express yourself and make your documents seem professional with custom text added in, or tweak the file's original input to excellence - all comes along with the capability to insert your personal graphics and sign it off.
It is straightforward to fill out the pdf using out detailed tutorial! Here's what you want to do:
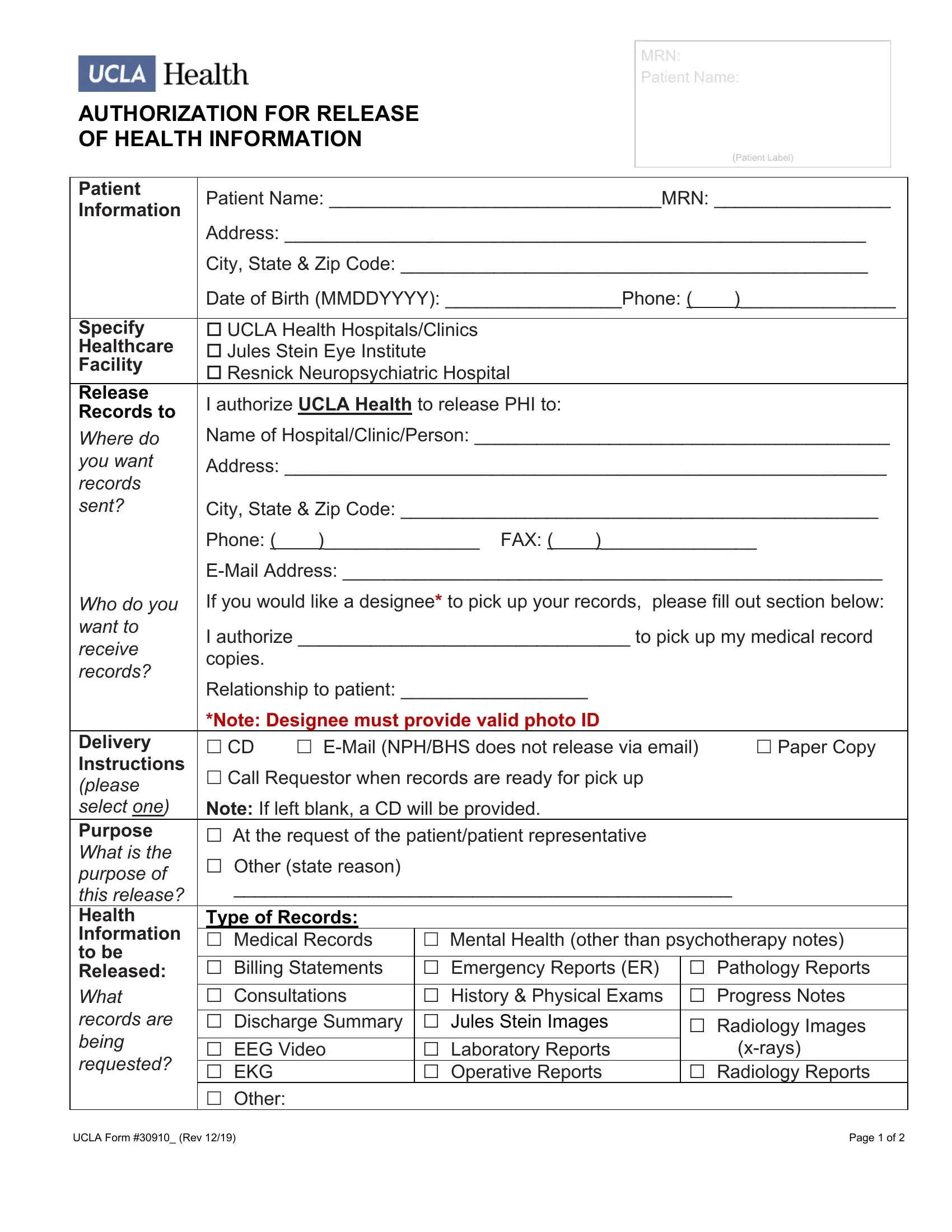
1. You will need to fill out the ucla medical reports accurately, hence take care when working with the areas that contain all these blanks:
2. Your next stage is to complete all of the following blank fields: Where do you want records sent, Who do you want to receive records, Delivery Instructions please, City State Zip Code, Phone FAX, EMail Address, If you would like a designee to, I authorize to pick up my medical, Relationship to patient, Note Designee must provide valid, EMail NPHBHS does not release via, Paper Copy, Call Requestor when records are, Note If left blank a CD will be, and Other state reason.
3. The following portion is mostly about Delivery Instructions please, Mental Health other than, Type of Records Medical Records, Radiology Images, xrays, Radiology Reports, UCLA Form Rev, and Page of - fill out all these blank fields.
4. This next section requires some additional information. Ensure you complete all the necessary fields - AUTHORIZATION FOR RELEASE OF, MRN Patient Name, Patient Label, Sensitive Information, Specify DateTime Period Expiration, Signatures, Sensitive information will not be, Genetic Testing Information, FROM MM DD YYYY TO MM DD YYYY, Unless otherwise revoked this, Signature of Patient Legal, and Printed Name Area CodePhone - to proceed further in your process!
As for FROM MM DD YYYY TO MM DD YYYY and MRN Patient Name, be sure that you review things in this current part. Both of these are viewed as the most significant fields in this PDF.
5. The very last stage to submit this document is pivotal. Be sure you fill out the appropriate blank fields, particularly If signed by someone other than, patient, Signature of Witness only if, Mailing Addresses Please check, and Please check box for radiology, prior to using the file. In any other case, it could result in an unfinished and probably invalid document!
Step 3: Spell-check what you've entered into the blank fields and then hit the "Done" button. Join us today and immediately access ucla medical reports, prepared for download. All alterations you make are saved , allowing you to change the file at a later point when necessary. Here at FormsPal, we endeavor to be certain that your information is maintained private.