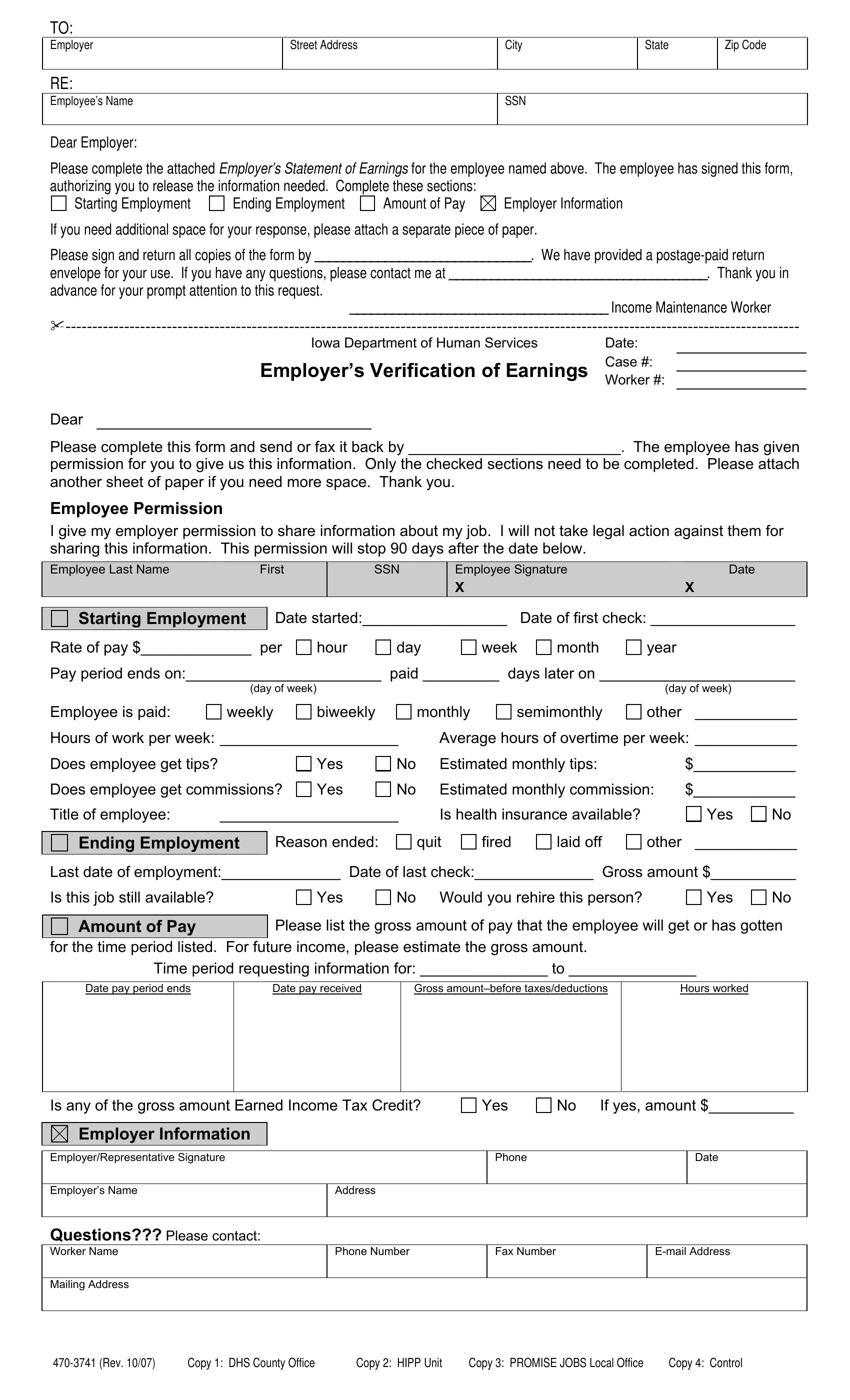
In the multifaceted world of employment and social services, the Employer Verification of Earnings form serves as a vital tool to ensure the accuracy and integrity of financial information provided by employees to various governmental or institutional bodies. Originating from the Iowa Department of Human Services, this document facilitates a structured method for employers to report earnings of their workforce when requested, exemplifying a commitment to transparent and responsible information sharing. Through sections that detail starting and ending employment, amount of pay, and employer specifics, the form encapsulates a comprehensive overview of an individual’s employment journey. Further emphasizing its utility, it includes permissions for the release of this data signed by the employee, thereby safeguarding against legal repercussions and fostering a respectful exchange of personal financial data. Designed to be filled out with ease and returned using a provided postage-paid envelope, the process aims for efficiency and convenience for both parties involved. Moreover, the option to attach additional sheets ensures that complex employment histories can be accommodated without compromise, rounding off a document that is both thorough in its purpose and considerate in its execution.
| Question | Answer |
|---|---|
| Form Name | Employer Verification Of Earnings Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | employment verification of earnings form wisconsin, employer verification of earnings pdf, employment verification form wisconsin, employment verification form pdf wisconsin |
