In order to ensure employees are being paid the correct amount, most businesses require a form for verifying employee earnings. This form can be used to confirm the number of hours an employee has worked, as well as their pay rate. The information on this form can help employers ensure that they are in compliance with all wage and hour laws. If you are an employer looking for more information on how to complete an earnings verification form, or if you are an employee who needs to download one, keep reading.
| Question | Answer |
|---|---|
| Form Name | Earnings Verification Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | earnings verification form, employment verification form for food stamps, earnings verification online, employment verification form for welfare |
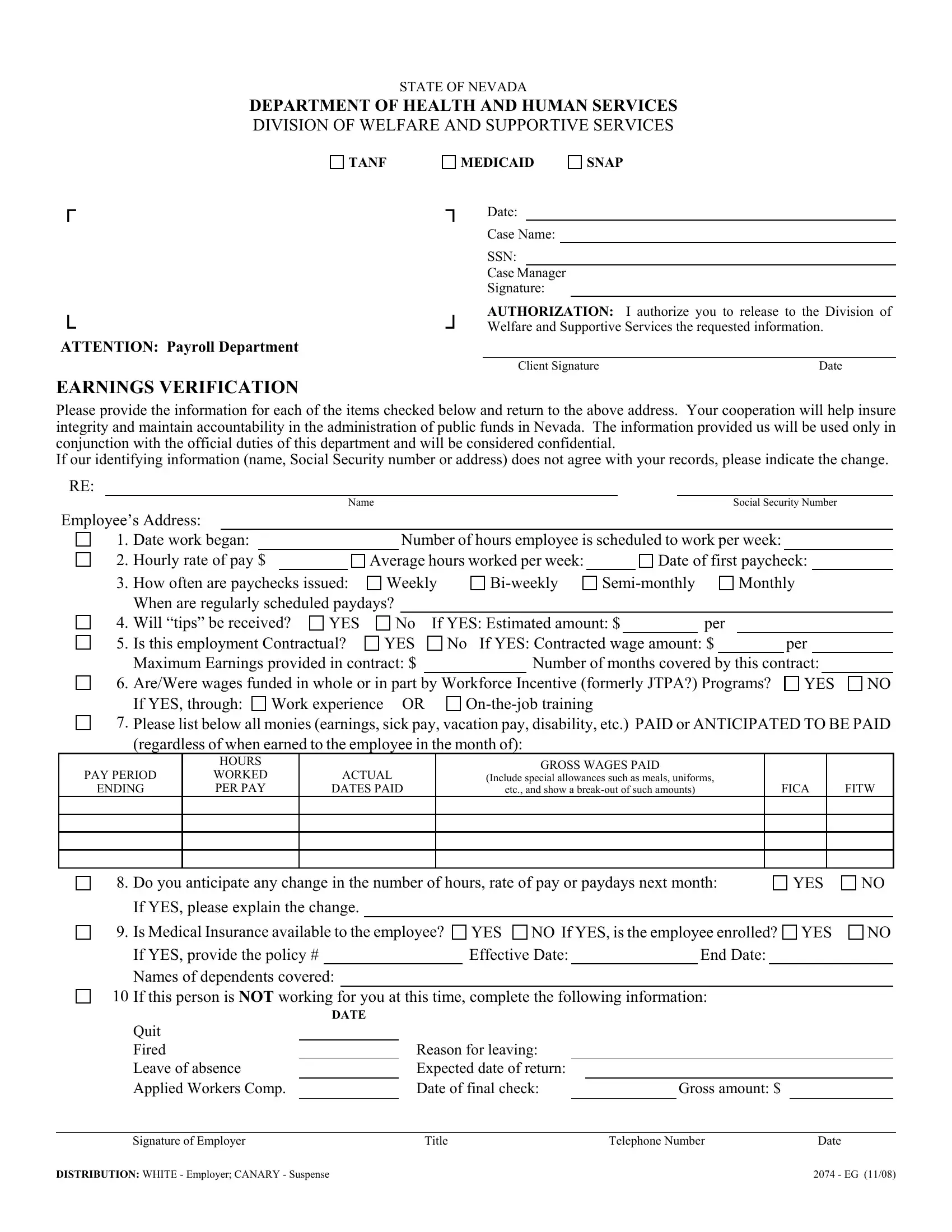
STATE OF NEVADA
DEPARTMENT OF HEALTH AND HUMAN SERVICES
DIVISION OF WELFARE AND SUPPORTIVE SERVICES
TANF
┌
└
ATTENTION: Payroll Department
MEDICAID |
SNAP |
┐Date:
Case Name:
SSN:
Case Manager Signature:
┘ |
AUTHORIZATION: I authorize you to release to the Division of |
|
Welfare and Supportive Services the requested information. |
||
|
|
|
|
Client Signature |
Date |
EARNINGS VERIFICATION
Please provide the information for each of the items checked below and return to the above address. Your cooperation will help insure integrity and maintain accountability in the administration of public funds in Nevada. The information provided us will be used only in conjunction with the official duties of this department and will be considered confidential.
If our identifying information (name, Social Security number or address) does not agree with your records, please indicate the change.
RE:
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
Social Security Number |
|
||||
Employee’s Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. |
Date work began: |
|
|
|
|
|
|
Number of hours employee is scheduled to work per week: |
|
|
|
|
||||||||||||
2. |
Hourly rate of pay $ |
|
|
|
Average hours worked per week: |
|
|
|
Date of first paycheck: |
|
|
|||||||||||||
3. |
How often are paychecks issued: |
Weekly |
|
Monthly |
|
|||||||||||||||||||
|
When are regularly scheduled paydays? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
4. |
Will “tips” be received? |
YES |
No If YES: Estimated amount: $ |
|
|
per |
|
|
|
|
|
|
||||||||||||
5. |
Is this employment Contractual? |
YES |
No If YES: Contracted wage amount: $ |
|
|
|
per |
|
|
|||||||||||||||
|
Maximum Earnings provided in contract: $ |
|
|
Number of months covered by this contract: |
|
|
||||||||||||||||||
6. |
Are/Were wages funded in whole or in part by Workforce Incentive (formerly JTPA?) Programs? |
YES |
NO |
|||||||||||||||||||||
|
If YES, through: |
Work experience |
|
OR |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
7. |
Please list below all monies (earnings, sick pay, vacation pay, disability, etc.) PAID or ANTICIPATED TO BE PAID |
|||||||||||||||||||||||
|
(regardless of when earned to the employee in the month of): |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
PAY PERIOD
ENDING
HOURS
WORKED PER PAY
ACTUAL
DATES PAID
GROSS WAGES PAID
(Include special allowances such as meals, uniforms,
etc., and show a
FICA
FITW
8. |
Do you anticipate any change in the number of hours, rate of pay or paydays next month: |
YES |
NO |
|
||||||||||||
|
If YES, please explain the change. |
|
|
|
|
|
|
|
|
|
|
|
|
|||
9. |
Is Medical Insurance available to the employee? |
YES |
NO If YES, is the employee enrolled? |
YES |
NO |
|
||||||||||
|
If YES, provide the policy # |
|
|
Effective Date: |
|
|
|
End Date: |
|
|
|
|
||||
|
Names of dependents covered: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
10 |
If this person is NOT working for you at this time, complete the following information: |
|
|
|
||||||||||||
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
||
|
Quit |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Fired |
|
Reason for leaving: |
|
|
|
|
|
|
|
|
|||||
|
Leave of absence |
|
Expected date of return: |
|
|
|
|
|
|
|
|
|||||
|
Applied Workers Comp. |
|
Date of final check: |
|
|
Gross amount: $ |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
Signature of Employer |
Title |
|
|
|
Telephone Number |
Date |
|
|
|||||||
DISTRIBUTION: WHITE - Employer; CANARY - Suspense |
2074 - EG (11/08) |