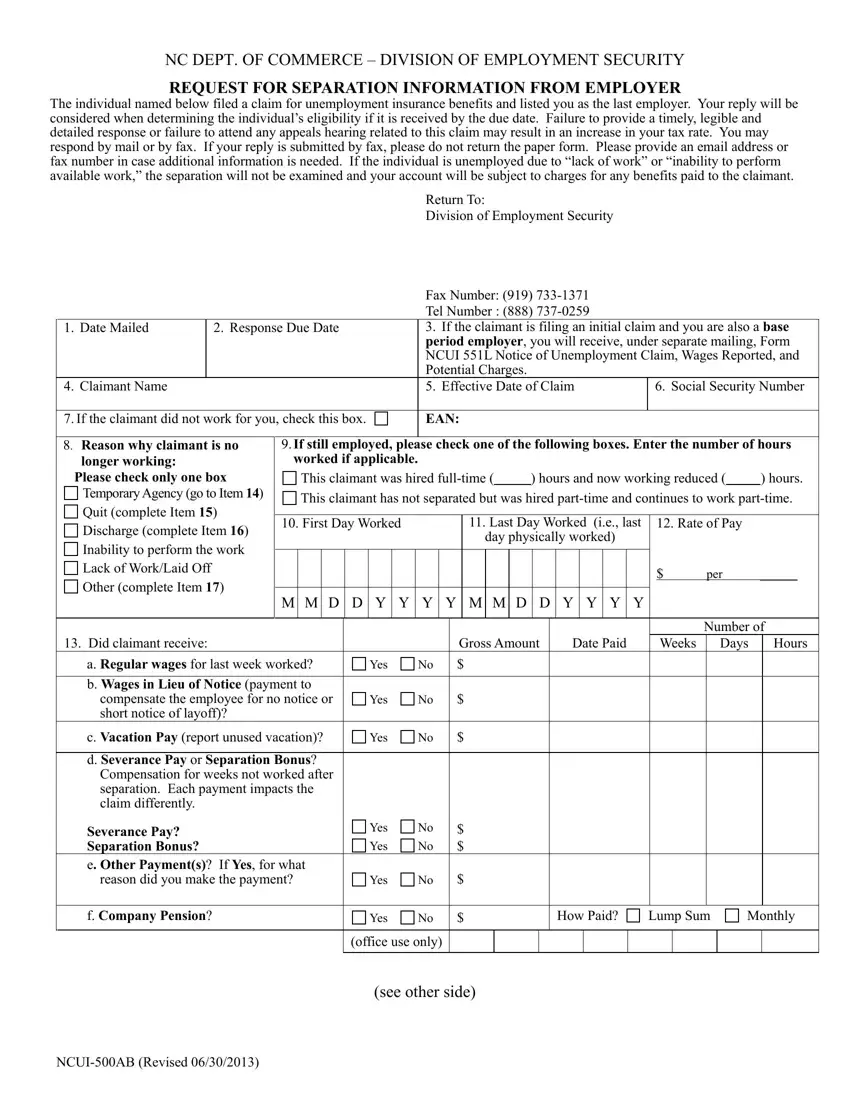
At the heart of managing unemployment insurance benefits claims lies the intricate process facilitated by the Unemployment Commission Form, specifically designed by the NC Department of Commerce – Division of Employment Security. This form serves as a critical link between former employers and the Division, requesting detailed separation information following a claim filed by an individual for unemployment benefits. The form emphasizes the importance of a punctual, readable, and comprehensive reply from employers, outlining that failure to respond adequately or attend any appeals hearing may lead to an increased tax rate for the employer. Additionally, it provides options to respond via mail or fax, discouraging the return of the paper form if the fax option is chosen and suggesting the provision of an email or fax number for any further correspondence. This form intricately categorizes reasons for the employee's unemployment and seeks specific details such as the effective date of the claim, social security number, first and last day worked, and types of payment the claimant received, among others. For temporary employment services employers, it specifies how to report on claimants who are not separated but for whom no suitable work assignments are available. Furthermore, it guides through the process of reporting if a claimant has quit or was discharged, necessitating detailed documentation of reasons, prior notifications, and any policy violations. The careful completion of this form plays a pivotal role in determining the eligibility of individuals for unemployment benefits, guarding against undue charges on the employer’s account and ensuring the integrity of the unemployment insurance system.
| Question | Answer |
|---|---|
| Form Name | Unemployment Commission Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | nc clm 500ab, ncu1500ab form, form ncui 551l, nc clm 500 ab |
