Navigating the complexities of applying for Unemployment Insurance can seem daunting, but understanding the application form and its requirements is the first step towards obtaining the benefits you rightly deserve. The form, designed for meticulous scrutiny by the Department of Employment Development, requires applicants to provide detailed personal and employment information, including Social Security numbers, previous employment details over the last 18 months, and reasons for unemployment. Accuracy is paramount, as incorrect or incomplete information can lead to delays or denials of claims. Applicants are advised to use blue or black ink and ensure that all sections are comprehensively filled out. This includes disclosing any employment outside the state or in Canada, a thorough account of your last employment, and insight into your personal situation such as any disabilities, your highest level of education, and specific details about your circumstances leading to unemployment. In addition, the form questions aim to capture a snapshot of the applicant's readiness and availability for work, preferences for communication, and any linguistic needs that should be accommodated, making this document a comprehensive tool for both the applicant and the reviewing officials.
| Question | Answer |
|---|---|
| Form Name | Unemployment Insurance Application Form |
| Form Length | 12 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min |
| Other names | de1101i, 1997, California, printable california unemployment application |
For Department Use Only
Date Received:
Date Postmarked/Faxed:
Effective Date:
UNEMPLOYMENT INSURANCE APPLICATION
FILING INSTRUCTIONS
Complete this application including any applicable attachment(s). Print or type the information. Use blue or black ink only.
Answer all questions on each page. Review your application thoroughly for completeness. An incomplete application may delay or prevent the filing of your claim, or cause benefits to be denied. If the Employment Development Department (EDD) needs to verify any of the information you provide while filing a claim, you will receive additional forms by mail and will be asked to provide additional information and/or documentation.
APPLICATION QUESTIONS
The answers you give to the questions on this application must be true and correct. You may be subject to penalties if you make a false statement or withhold information.
1. |
Did you work in a state other than California during the |
1. |
|
|
Yes |
No |
If yes, check the applicable box(es) below: |
|
|
|||||||||||||
|
last 18 months? |
|
|
|
State(s) Outside California, specify state(s): |
|
|
|||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||
|
AND / OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Did you work in Canada during the last 18 months? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Canada |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
What is your Social Security number as given to you by |
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the Social Security Administration? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If the EDD assigned you an EDD Client Number |
|
|
a) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(ECN), please provide the ECN here. (An ECN is a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2A. |
List any other Social Security numbers you have used. |
2A. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
3. |
What is your full name? |
3. |
|
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Middle Initial |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
4. |
Is this the name that appears on your Social Security |
4. |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|||||
|
card? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If no, provide the name that appears on your Social |
|
|
a) |
|
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Security card. |
|
|
|
|
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
Middle Initial |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
List any other names you have used. |
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
What is your birth date? |
6. |
|
|
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
7. |
What is your gender? |
7. |
|
|
|
Male |
|
|
Female |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
8. |
Would you prefer your written material in English or |
8. |
|
|
|
English |
|
|
Spanish |
|
|
|||||||||||
|
Spanish? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) What is your preferred spoken language? |
|
|
a) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
9. |
Have you filed a California Unemployment Insurance or a |
9. |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|||||
|
Disability Insurance claim in the last two years? |
|
|
a) Unemployment Claim Date(s) (mm/dd/yyyy) |
|
|
||||||||||||||||
|
|
|
|
|
|
|||||||||||||||||
|
a) If yes, list each type of claim and the most recent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
date(s) of when the claim(s) was filed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) |
|
Disability Claim Date(s) (mm/dd/yyyy) |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 1 of 12 |
CU |
UNEMPLOYMENT INSURANCE APPLICATION
|
|
|
Social Security Number: |
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. Do you have a Driver’s License issued to you by a |
10. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
State/entity? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If yes, provide the name of the issuing State/entity and |
|
|
a) |
Name of issuing State/entity: |
|
|
|
|
|
|
|
|
|
|||||||||||||
your Driver’s License number. |
|
|
|
|
Driver’s License Number: |
|
|
|
|
|
|
|
|
|
|
|||||||||||
If no, answer questions |
|
|
|
|
If no, answer questions |
|
|
|
|
|
|
|
|
|
||||||||||||
b) Do you have an Identification Card issued to you by a |
|
|
b) |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
State/entity? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c) If yes, provide the name of the issuing State/entity and |
|
|
c) |
Name of issuing State/entity: |
|
|
|
|
|
|
|
|
|
|||||||||||||
your Identification Card number. |
|
|
|
|
Identification Card Number: |
|
|
|
|
|
|
|
|
|
||||||||||||
d) How do you look for work and, if you have work, how |
|
|
d) |
Please Explain: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
do you get to work? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. What is your telephone number? |
|
11. |
|
|
- |
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If you are deaf, hard of hearing, or have a speech |
|
|
a) |
|
TTY |
|
California Relay Service |
|
|
|
|
|||||||||||||||
disability and use TTY or California Relay to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
communicate, check the appropriate box. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
12. What is your mailing address? |
|
12. |
|
Street: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Apt. |
|
_ |
|
|
|
|||
(Include your city, State, and ZIP code) |
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
State: |
ZIP Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
13. Is your residence address the same as your mailing |
13. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
address? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If no, enter your residence address. (Include your city, |
|
|
a) |
Street: |
|
|
|
|
|
|
|
|
|
|
|
|
Apt. |
_ |
|
|
|
|||||
State, ZIP code and apartment number.) A residence |
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
address cannot be a P.O. Box. Please provide a street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
address. |
|
|
|
|
State: |
ZIP Code: |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. If you do not live in California, what is the name of the |
14. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County in which you live? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
15. What race or ethnic group do you identify with? Check one of the following: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
White |
Black not Hispanic |
|
|
|
|
|
|
|
|
|
Hispanic |
|
|
|
|
|
|
|
|
|
||||||
Asian |
American Indian/Alaskan Native |
Chinese |
|
|
|
|
|
|
|
|
|
|||||||||||||||
Cambodian |
Filipino |
|
|
|
|
|
|
|
|
|
|
Other Pacific Islander |
|
|
|
|
||||||||||
Guamanian |
Asian Indian |
|
|
|
|
|
|
|
|
|
|
Japanese |
|
|
|
|
|
|
|
|
|
|||||
Korean |
Laotian |
|
|
|
|
|
|
|
|
|
|
Samoan |
|
|
|
|
|
|
|
|
|
|||||
Vietnamese |
Hawaiian |
|
|
|
|
|
|
|
|
|
|
I choose not to answer |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
16. Do you have a disability? (A disability is a physical or |
16. |
|
|
Yes |
No |
I choose not to answer |
|
|
|
|
||||||||||||||||
mental impairment that substantially limits one or more life |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
activities, such as caring for oneself, performing manual |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
tasks, walking, seeing, hearing, speaking, breathing, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
learning, or working.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
17. What is the highest grade of school you have completed? Check only one box. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Did not complete High School |
High School Diploma or GED |
|
|
|
Some college or vocational school |
|
|
|
|
|||||||||||||||||
Associate of Arts |
Bachelor of Arts or Science |
|
|
|
Masters or Doctorate |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
18. Are you a Military Veteran? |
|
18. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
DE 1101ID Rev. 3 |
Page 2 of 12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
UNEMPLOYMENT INSURANCE APPLICATION
Social Security Number:
19.Provide your employment and wages information for the past 18 months. If you worked for a temporary agency, a labor contractor, an agent for actors or actresses, or an employer where wages are reported under a corporate name, your wages may have been reported under that employer name. You may want to refer to your check stub(s) or
a)Name and mailing address of all employers you worked for in the last 18 months.
b)Period of employment (Dates Worked).
c)Total Wages earned for each employer in the last 18 months.
d)How you were paid (specify hourly, weekly, monthly, annually, commission, or at piece rate).
e)Specify if you worked
f)How many hours you worked per week.
g)Check the appropriate “Yes/No” box if the employer is (or is not) a school or educational institution or a public or nonprofit employer where you performed
NOTE: It is important that you report the employer name(s) and mailing address(es), period(s) of employment, and wages correctly. Failure to provide complete information will result in your benefits being delayed or denied.
a) Employer Name and Mailing Address |
b) Dates Worked |
c) Total Wages |
d) How were you paid? (e.g., |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
weekly, monthly, etc.)? |
Name: |
|
|
|
|
From: |
|
$ |
|
|
|
||
Mailing Address: |
To: |
|
|
|
|
|||||||
Street: |
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
ZIP Code: |
|
|
|
|
|
|
|
|
|
e) Did you work |
F/T |
P/T |
f) How many hours did you work per week? |
g) Is this employer a school employer or a public or nonprofit employer where you performed
If yes, provide phone number |
- |
- |
Yes
No
a) Employer Name and Mailing Address |
b) Dates Worked |
c) Total Wages |
d) How were you paid? (e.g., |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
weekly, monthly, etc.)? |
Name: |
|
|
|
|
From: |
|
$ |
|
|
|
||
Mailing Address: |
To: |
|
|
|
|
|||||||
Street: |
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
ZIP Code: |
|
|
|
|
|
|
|
|
|
e) Did you work |
F/T |
P/T |
f) How many hours did you work per week? |
g) Is this employer a school employer or a public or nonprofit employer where you performed
If yes, provide phone number |
- |
- |
Yes
No
a) Employer Name and Mailing Address |
b) Dates Worked |
c) Total Wages |
d) How were you paid? (e.g., |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
weekly, monthly, etc.)? |
Name: |
|
|
|
|
From: |
|
$ |
|
|
|
||
Mailing Address: |
To: |
|
|
|
|
|||||||
Street: |
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
ZIP Code: |
|
|
|
|
|
|
|
|
|
e) Did you work |
F/T |
P/T |
f) How many hours did you work per week? |
g) Is this employer a school employer or a public or nonprofit employer where you performed
If yes, provide phone number |
- |
- |
Yes
No
a) Employer Name and Mailing Address |
b) Dates Worked |
c) Total Wages |
d) How were you paid? (e.g., |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
weekly, monthly, etc.)? |
Name: |
|
|
|
|
From: |
|
$ |
|
|
|
||
Mailing Address: |
To: |
|
|
|
|
|||||||
Street: |
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
ZIP Code: |
|
|
|
|
|
|
|
|
|
e) Did you work |
F/T |
P/T |
f) How many hours did you work per week? |
g) Is this employer a school employer or a public or nonprofit employer where you performed
If yes, provide phone number |
- |
- |
Yes
No
DE 1101ID Rev. 3 |
Page 3 of 12 |
UNEMPLOYMENT INSURANCE APPLICATION
Social Security Number:
19.Continued
a) Employer Name and Mailing Address |
b) Dates Worked |
c) Total Wages |
d) How were you paid? (e.g., |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
weekly, monthly, etc.)? |
Name: |
|
|
|
|
From: |
|
$ |
|
|
|
||
Mailing Address: |
To: |
|
|
|
|
|||||||
Street: |
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
ZIP Code: |
|
|
|
|
|
|
|
|
|
e) Did you work |
F/T |
P/T |
f) How many hours did you work per week? |
g) Is this employer a school employer or a public or nonprofit employer where you performed
If yes, provide phone number |
- |
- |
Yes
No
a) Employer Name and Mailing Address |
b) Dates Worked |
c) Total Wages |
d) How were you paid? (e.g., |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
weekly, monthly, etc.)? |
Name: |
|
|
|
|
From: |
|
$ |
|
|
|
||
Mailing Address: |
To: |
|
|
|
|
|||||||
Street: |
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
ZIP Code: |
|
|
|
|
|
|
|
|
|
e) Did you work |
F/T |
P/T |
f) How many hours did you work per week? |
g) Is this employer a school employer or a public or nonprofit employer where you performed
If yes, provide phone number |
- |
- |
Yes
No
20. |
During the past 18 months did you work for any other |
20 |
Yes |
No |
||||
|
employers not listed in question 19? |
If yes, list the employer information for questions 19 |
||||||
|
|
|||||||
|
|
sheet of paper. Attach the additional sheet of paper to this application. |
||||||
|
|
|
|
|
|
|
|
|
21. |
If the EDD finds that you do not have sufficient wages in |
21 |
Yes |
No |
||||
|
the Standard Base Period to establish a valid claim, do |
|
|
|
|
|
|
|
|
you want to attempt to establish a claim using the |
|
|
|
|
|
|
|
|
Alternate Base Period? |
|
|
|
|
|
|
|
|
For additional information about the Standard Base Period |
|
|
|
|
|
|
|
|
and the Alternate Base Period, visit the EDD website |
|
|
|
|
|
|
|
|
www.edd.ca.gov. |
|
|
|
|
|
|
|
|
|
|
|
|||||
22. |
During the past 18 months, which employer did you work |
22. Employer name: |
||||||
|
for the longest? |
|
|
|
|
|
|
|
|
a) What type of business was operated by the employer? |
|
a) Type of business: |
|||||
|
(Please be specific. For example, restaurant, dry |
|
|
|
|
|
|
|
|
cleaning, construction, book store.) |
|
|
|
|
|
|
|
|
b) How long did you work for that employer? |
|
b) Years |
Months |
||||
|
c) What type of work did you do for that employer? |
|
c) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23. |
What is your usual occupation? |
23. |
|
|
|
|
|
|
|
|
|
|
|
||||
24. |
Is your usual work seasonal? |
24. |
Yes |
No |
||||
|
If yes, answer questions |
|
If yes, answer questions |
|||||
|
a) When does the season usually begin? |
|
a) |
|
|
|
(mm/dd/yyyy) |
|
|
b) When does the season usually end? |
|
b) |
|
|
|
(mm/dd/yyyy) |
|
|
c) What other |
|
c) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 4 of 12 |
UNEMPLOYMENT INSURANCE APPLICATION
Social Security Number:
Please provide information about your very last employer. This is the employer you last worked for regardless of the length of time you worked at that job, the type of work you did for that employer, or whether or not you have been paid.
If you worked for a temporary agency, a labor contractor, an agent for actors or actresses, or an employer where wages are reported under a corporate name, your wages may have been reported under that employer name. If you worked for
Reminder: To file a claim, individuals must be out of work or working less than full time. You must provide information about the last employer you worked for as an employee. Do not include
25. What is the last date you actually worked for your very |
|
|
25. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|||||||||||||
last employer? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
a) |
What are your gross wages for your last week of work? |
|
|
a) $ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
For Unemployment Insurance purposes, a week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
begins on Sunday and ends the following Saturday. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
b) |
What is the complete name of your very last |
|
|
|
|
b) Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
employer? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
c) |
What is the mailing address of your very last |
|
|
|
|
c) |
Mailing address: |
|
|
|
|||||||||||||||||||||||||
|
employer? |
|
|
|
|
|
|
|
|
Street: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
|
ZIP Code: |
|
|
|
|
|
|||||||||||||
d) |
Is the physical address of your very last employer the |
|
|
d) |
|
|
Yes |
|
|
|
No |
|
|
|
|||||||||||||||||||||
|
same as their mailing address? (A physical address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
cannot be a P.O. Box. Please provide a street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
address.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
If no, what is the physical address of your very last |
|
|
|
Physical address: |
|
|
|
||||||||||||||||||||||||||
|
|
employer? |
|
|
|
|
|
|
|
|
Street: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
|
ZIP Code: |
|
|
|
|
|
|||||||||||||
e) |
What is the telephone number of your very last |
|
|
|
e) |
- |
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
employer at their physical address? |
|
|
|
|
|
f) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
f) |
What is the name of your immediate supervisor? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
g) |
Briefly explain in your own words the reason you are |
|
|
g) Reason: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
no longer working for your very last employer, within |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
the space provided. Please do not include any |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
attachments. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26. Are you (directly or indirectly) out of work with any employer |
26 |
|
|
Yes |
No |
|
|
|
|||||||||||||||||||||||||||
(last employer or any employer in the last 18 months) due to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
a trade dispute, such as a strike or a lockout? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
If yes and a union was/is involved, answer questions |
|
|
If yes and a union was not/is not involved, answer questions |
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
a) What is the name and telephone number of the union? |
c) |
How many employees left work? |
|
|
|
|
|
||||||||||||||||||||||||||||
Name: |
|
|
|
|
|
|
|
d) Was there a spokesperson for the employees? |
Yes |
No |
|
||||||||||||||||||||||||
Phone: |
- |
- |
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
e) |
If yes, what is his/her name and telephone number? |
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
b) Are you going to receive strike benefits? |
Yes |
No |
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Phone: |
- |
- |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 5 of 12 |

UNEMPLOYMENT INSURANCE APPLICATION
|
|
Social Security Number: |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
27. Are you currently working for or do you expect to work for |
27. |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
any school or educational institution or a public or nonprofit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
employer performing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, answer questions |
If yes, answer questions |
|
|
||||||||||||||
a) Provide the following information for the school or |
a) |
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
educational institution(s) or the public or nonprofit |
|
Mailing Address: |
|
|
|
|
|
|
|
|
||||||
|
employer(s). |
|
Street: |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
ZIP Code: |
|
|
|
|
||||||
|
|
|
Phone: |
- |
|
- |
|
|
|
|
|
|
|
||||
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Mailing Address: |
|
|
|
|
|
|
|
|
||||||
|
|
|
Street: |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
ZIP Code: |
|
|
|
|
||||||
|
|
|
Phone: |
- |
|
- |
|
|
|
|
|
|
|
||||
b) Are you a substitute teacher for Los Angeles |
b) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
|
Unified School District (LAUSD)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c) Are you currently in a recess period or off track? |
c) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
d) Do you have reasonable assurance to return to |
d) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
|
work after the recess period or the off track period |
|
If yes, when? |
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|||||
|
with any school or educational institution? |
|
|
|
|
|
|
|
|
||||||||
|
e) |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
||||||
e) What is the beginning date of your next recess or |
|
|
|
|
|
|
|
|
|
||||||||
|
the next off track period? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
28. Do you expect to return to work for any former employer? |
28. |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
29. Do you have a date to start work with any employer? |
29. |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
If yes, answer question a: |
If yes, answer question a: |
|
|
||||||||||||||
a) What date will you start work? |
a) |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
30. Are you a member of a union? |
30. |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
If yes, answer questions |
If yes, answer questions |
|
|
||||||||||||||
a) |
What is your union name and local number? |
a) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b) |
Are you in good standing with your union? |
b) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|||
c) Does your union look for work for you? |
c) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
d) Does your union control your hiring? |
d) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||||
e) |
Are you registered with your union as out of work? |
e) |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 6 of 12 |

UNEMPLOYMENT INSURANCE APPLICATION
|
|
Social Security Number: |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31. |
Are you currently attending, or do you plan on attending |
31. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
||||
|
school or training? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, answer question |
|
If yes, answer questions |
|
|
|
|
|||||||||||
|
a) What is the starting date of the school or training? |
|
a) |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|||
|
b) What is the ending date of the current session? |
|
b) |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|||
|
c) What is the name of the school? |
|
c) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d) What is the telephone number of the school? |
|
d) Phone: |
- |
|
|
|
- |
|
|
|
|
|
|
|
|||
|
e) What are the days and hours you are attending, or |
|
e) Days and hours: |
|
|
|
|
|
|
|
|
|||||||
|
plan to attend, school? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f) Is your school or training program authorized or funded |
|
f) |
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
||
|
by one of the programs listed in section f? |
If yes, check only one box. |
|
|
|
|
||||||||||||
|
NOTE: If you completed apprenticeship training, |
|
|
|
Workforce Investment Act (WIA) |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
Employment Training Panel (ETP) |
|
|
|
|
||||||||||
|
complete questions |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
Trade Adjustment Assistance (TAA) |
|
|
|
|
||||||||||
|
certificate with your CONTINUED CLAIM FORM, |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
California Work Opportunity and Responsibility to Kids |
|
|
|
|
||||||||||
|
DE 4581, for the week(s) of training. |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
(CalWORKS) |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
Union Apprenticeship |
|
|
|
|
|||||||||
|
|
|
|
|
Union Journey Level |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32. |
Are you available for immediate |
32. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
||||
|
usual occupation? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If no, please explain why you are not available for |
|
a) |
|
Explanation: |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
33. |
Are you available for immediate |
33. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
||||
|
usual occupation? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If no, please explain why you are not available for |
|
a) |
|
Explanation: |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. |
Are you currently |
34. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
||||
|
become |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
have your own business or work as an independent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
contractor.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
35. Are you now, or have you been in the last 18 months an |
35. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|||||
|
officer of a corporation or union or the sole or major |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
stockholder of a corporation? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a) If yes, include name of organization and your title or |
|
a) |
|
Name of Organization: |
|
|
|
|
|||||||||
|
position. |
|
|
|
Title/Position: |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36. |
Did you serve as an elected public official or Governor- |
36. |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
||||
|
exempt appointee in the last 18 months? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 7 of 12 |
UNEMPLOYMENT INSURANCE APPLICATION
|
Social Security Number: |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. Are you currently receiving a pension? |
37. |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||||
If yes, answer question a: |
If yes, answer question a: |
|
|
|
|
|
|||||||||||
a) Are you currently receiving more than one pension? |
a) |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||
If yes, proceed to question 38. |
|
If yes, proceed to question 38. |
|
|
|
|
|
||||||||||
If no, answer questions |
|
If no, answer questions |
|
|
|
|
|
||||||||||
b) What is the name of the pension provider? |
b) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c) Is the pension based on another person’s work or |
c) |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||
wages? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d) Is the pension a union pension or a pension funded by |
d) |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||
more than one employer? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e) What is the name of the employer(s) paying into the |
e) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
pension? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f) Did you work for that employer in the last 18 months? |
f) |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38. Will you receive any additional pension(s) in the next |
38. |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||||
twelve months? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, answer questions |
If yes, answer questions |
|
|
|
|
|
|||||||||||
a) What is the name of the pension provider(s)? |
a) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b) When will you receive the pension(s)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
b) |
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
39. Are you receiving, or do you expect to receive, Workers’ |
39. |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||||
Compensation? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, answer questions |
If yes, answer questions |
|
|
|
|
|
|||||||||||
a) Who is the insurance carrier? |
a) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b) What is the insurance carrier’s telephone number? |
b) Phone: |
- |
|
- |
|
|
|
|
|
|
|
|
|
||||
c) What is the case number, if known? |
c) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d) What are the dates of your claim, if known? |
d) |
From: |
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
||||
|
|
|
|
To: |
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
||
|
|
|
|
|
|
|
|||||||||||
40. Have you received or do you expect to receive, any payments from your last employer, other than your |
Yes |
No |
|
|
|||||||||||||
regular salary? (Example: holiday pay, vacation pay, severance pay, |
|
|
|
|
|
||||||||||||
If yes, provide the information in sections
A. |
B. |
C. |
D. |
TYPE OF PAYMENT |
AMOUNT OF PAYMENT |
PAID FROM |
PAID TO |
(Example: vacation pay) |
(Example: $600) |
(Date: mm/dd/yyyy) |
(Date: mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 8 of 12 |
UNEMPLOYMENT INSURANCE APPLICATION
Social Security Number:
41.Are you a U. S. Citizen or National? If no, answer question a:
a)Are you registered with the United States Citizenship and Immigration Services (USCIS, formerly INS) and authorized to work in the United States?
b)Were you legally entitled to work in the United States for the last 19 months?
41. |
Yes |
No |
If no, answer question a:
a) |
Yes |
No |
b) |
Yes |
No |
IMPORTANT: If you answered “yes” to question “a” above, you must select one of the USCIS documents listed in 41A through 41H below and provide the applicable document information.
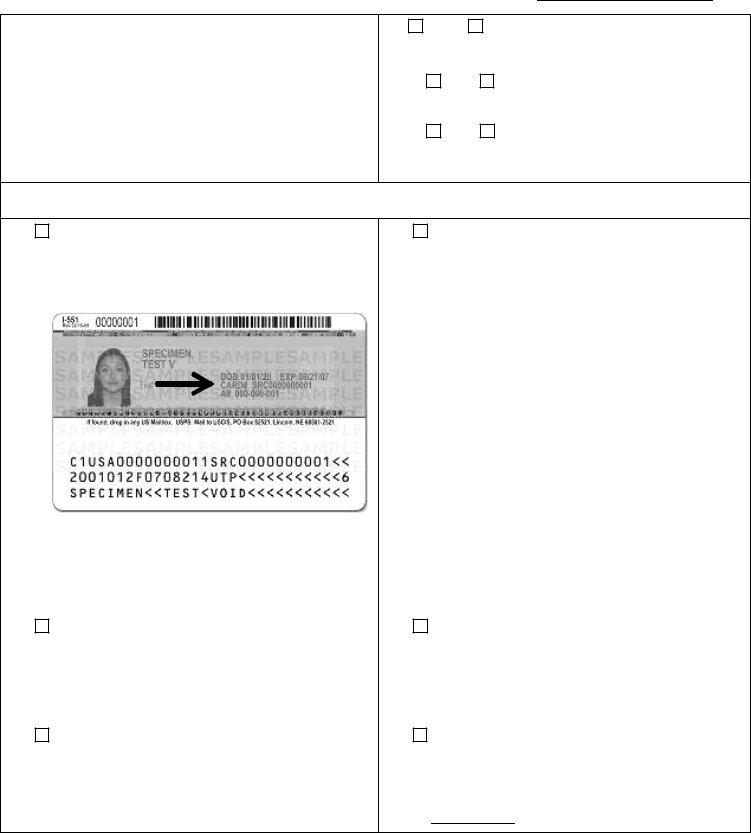
41A. Permanent Resident Card |
41A. Permanent Resident Card |
||||
1) |
Alien Registration Number (A#) |
1) A# |
|
|
|
|
|
The Alien Registration Number must be 7 to 9 digits long. |
|||
|
|
Enter numeric digits only. |
|||
2) |
Permanent Resident Card Number (CARD#) |
2) |
|
|
|
|
|
The CARD# must be 13 characters long. Enter 3 |
|||
|
|
alphabetic characters followed by 10 numeric digits. If your |
|||
|
|
current card was issued to you before December 1997, |
|||
|
|
leave this blank. |
|||
NOTE: The CARD# is on the back of the card, next to your photo, under the DOB and the EXP date.
3) |
Expiration Date (EXP) |
3) |
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|||||||
41B. Employment Authorization Card |
41B. Employment Authorization Card |
|||||||
1) |
Alien Registration Number (A#) |
1) |
A# |
|
|
|||
|
|
|
The Alien Registration Number must be 7 to 9 digits long. |
|||||
|
|
|
Enter numeric digits only. |
|||||
2) |
Expiration Date |
2) |
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|||||||
41C. Refugee Travel Document |
41C. Refugee Travel Document |
|||||||
1) |
Alien Registration Number (A#) |
1) |
A# |
|
|
|||
|
|
|
The Alien Registration Number must be 7 to 9 digits long. |
|||||
|
|
|
Enter numeric digits only. |
|||||
2) Expiration Date
2)(mm/dd/yyyy)
DE 1101ID Rev. 3 |
Page 9 of 12 |
UNEMPLOYMENT INSURANCE APPLICATION
|
|
|
Social Security Number: |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||
41D. |
Arrival/Departure Record |
|
41D. |
Arrival/Departure Record |
|||||||||
1) |
Arrival/Departure Number |
|
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Arrival/Departure Number must be 11 digits long. Enter |
|||||||||
|
|
|
|
numeric digits only. |
|||||||||
2) |
Expiration Date |
|
2) |
|
|
|
|
(mm/dd/yyyy) |
|||||
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|||||
41E. |
|
41E. |
|||||||||||
1) |
Alien Registration Number (A#) |
|
1) |
A# |
|
|
|||||||
|
|
|
|
The Alien Registration Number must be 7 to 9 digits long. |
|||||||||
|
|
|
|
Enter numeric digits only. |
|||||||||
2) |
Expiration Date |
|
2) |
|
|
|
|
(mm/dd/yyyy) |
|||||
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
||||||
41F. |
Unexpired Foreign Passport |
|
41F. |
Unexpired Foreign Passport |
|||||||||
1) |
Arrival/Departure Number |
|
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Arrival/Departure Number must be 11 digits long. Enter |
|||||||||
|
|
|
|
numeric digits only. |
|||||||||
2) |
Passport Number |
|
2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The passport number must be 6 to 12 alphanumeric |
|||||||||
|
|
|
|
characters. It is usually found on the top right corner of the |
|||||||||
|
|
|
|
document. |
|||||||||
3) |
Visa Number |
|
3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Visa Number must be 8 numeric digits. |
|||||||||
4) |
Expiration Date |
|
4) |
|
|
|
|
(mm/dd/yyyy) |
|||||
|
|
|
|
|
|
|
|||||||
41G. Arrival/Departure Record (I94) in Unexpired Foreign |
|
41G. Arrival/Departure Record (I94) in Unexpired Foreign |
|||||||||||
|
Passport |
|
|
Passport |
|||||||||
1) |
Arrival/Departure Number |
|
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Arrival/Departure Number must be 11 digits long. Enter |
|||||||||
|
|
|
|
numeric digits only. |
|||||||||
2) |
Passport Number |
|
2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The passport number must be 6 to 12 alphanumeric |
|||||||||
|
|
|
|
characters. It is usually found on the top right corner of the |
|||||||||
|
|
|
|
document. |
|||||||||
3) |
Visa Number |
|
3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Visa Number must be 8 numeric digits. |
|||||||||
4) |
Expiration Date |
|
4) |
|
|
|
|
(mm/dd/yyyy) |
|||||
|
|
|
|
|
|
||||||||
41H. Other Document (not listed in Section A to G) |
|
41H. Other Document (not listed in Section A to G) |
|||||||||||
1) |
Alien Registration Number (A#) |
|
1) |
A# |
|
|
|||||||
|
|
|
|
The Alien Registration Number must be 7 to 9 digits long. |
|||||||||
|
|
|
|
Enter numeric digits only. |
|||||||||
2) |
Arrival/Departure Number |
|
2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Arrival/Departure Number must be 11 digits long. Enter |
|||||||||
|
|
|
|
numeric digits only. |
|||||||||
3) |
Expiration Date |
|
3) |
|
|
|
|
(mm/dd/yyyy) |
|||||
4) |
Document Description |
|
4) |
Document Description: |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DE 1101ID Rev. 3 |
Page 10 of 12 |
|
|
|
|
|
|
|
|
|
|
||
UNEMPLOYMENT INSURANCE APPLICATION
Social Security Number:
SUPPLEMENTAL FORM FOR DISASTER UNEMPLOYMENT ASSISTANCE (DUA) – ATTACHMENT D
Please complete the following if you are unemployed or partially unemployed due to a disaster as you may be eligible for DUA benefits:
1.Are you unemployed as a direct result of a recent disaster in California, such as an earthquake, flood, mudslide, wildfire, etc.?
If yes:
a)Identify the type of disaster.
b)At the time of the disaster, in which county did you reside?
c)At the time of the disaster, in which county did you work?
d)At the time of the disaster, was your unemployment caused by your need to travel through a disaster area?
If yes:
Identify the disaster county or counties that prevent travel to your job.
e)Check the following that best applies to you:
f)If you selected item e1 or e3 above, how many hours did you work prior to the disaster?
g)If you selected e3 or e4 above briefly describe how the disaster affected your ability to continue or begin your
h)What is the physical address of your business?
1. |
Yes |
No |
If yes, answer questions
a)
b)
c)
d) |
Yes |
No |
e) 1) |
An employee who is unable to work as a direct result of |
|
the disaster. |
2) |
An individual who was scheduled to start work for an |
|
employer, but could not because of the disaster. |
3) |
A |
|
direct result of the disaster. |
4) |
An individual who intended to begin |
|
but could not because of the disaster. |
5) |
An individual who became head of household as a result |
of the disaster.
f)
g)
h)Street:
City:
State: |
|
Zip Code: |
DE 1101ID Rev. 3 |
Page 11 of 12 |

UNEMPLOYMENT INSURANCE APPLICATION
Social Security Number:
DO NOT MAIL OR FAX THIS PAGE
SUBMITTING YOUR APPLICATION
Be sure to review your application thoroughly for completeness. An incomplete application may delay or prevent the filing of your claim, or cause benefits to be denied.
Submit your completed application including any applicable attachment(s) by mail or fax:
By MAIL to the following address: |
EDD |
|
P.O. Box 12906 |
|
Oakland, CA |
|
NOTE: Extra postage is required. |
|
|
By FAX to the following telephone number: |
|
|
|
Once you submit your application, allow ten days for processing of your claim. You will receive Unemployment Insurance (UI) claim materials by mail. If you have not received any UI claim materials after ten days from the date you submitted your application, call one of the following
English |
Spanish |
Mandarin |
|
|
|
TTY (Non Voice) |
Cantonese |
Vietnamese |
|
|
|
Date Submitted: |
|
by |
Mail or
Fax
KEEP THIS PAGE FOR YOUR RECORDS
DE 1101ID Rev. 3 |
Page 12 of 12 |