Our top level software engineers worked hard to set-up the PDF editor we are now extremely pleased to deliver to you. This application enables you to quickly complete unitedhealthcare military veterns referral authorization request form and saves valuable time. You need to simply adhere to this specific procedure.
Step 1: To begin the process, choose the orange button "Get Form Now".
Step 2: After you have accessed the unitedhealthcare military veterns referral authorization request form editing page you can discover the whole set of functions you may carry out with regards to your document in the upper menu.
You'll have to enter the next details so that you complete the template:
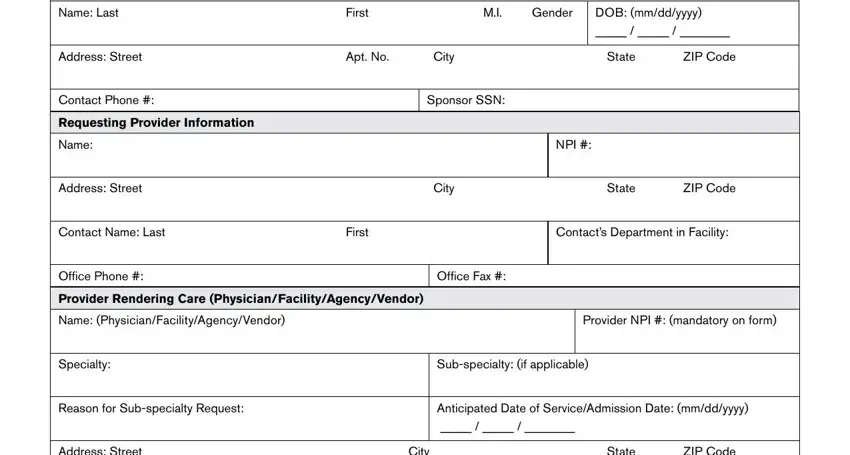
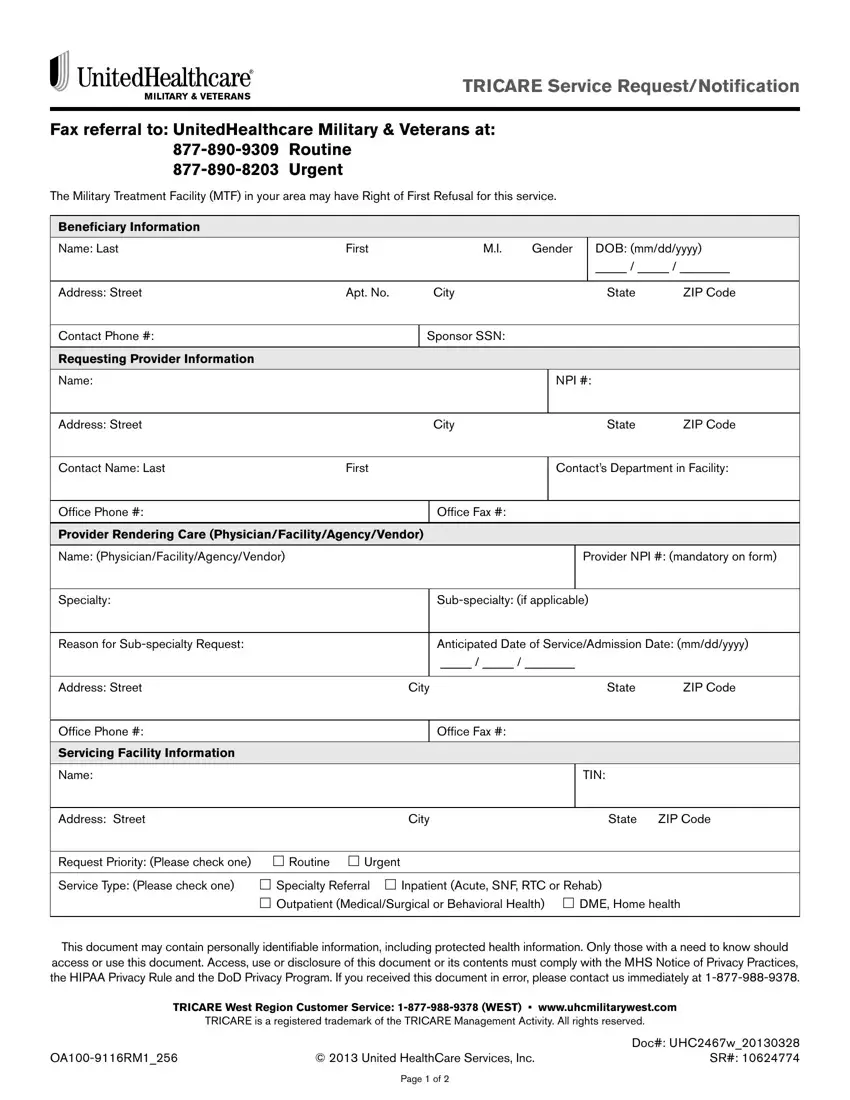
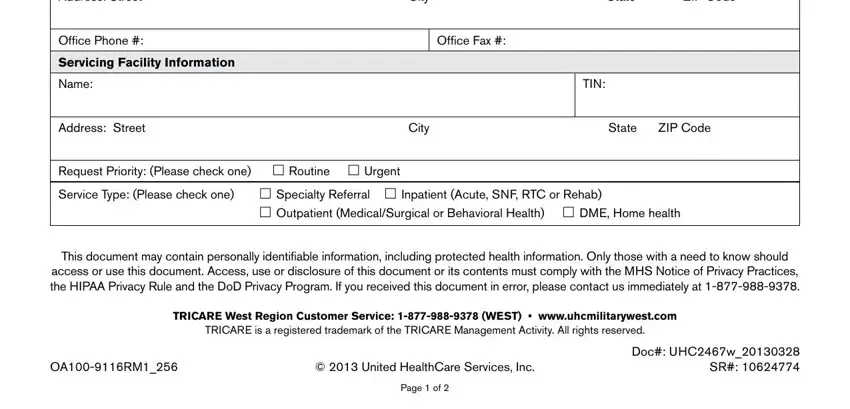
Provide the requested data in the field Address Street, City, State, ZIP Code, Office Phone, Servicing Facility Information, Name, Office Fax, TIN, Address Street, City, State, ZIP Code, Request Priority Please check one, and Outpatient MedicalSurgical or.
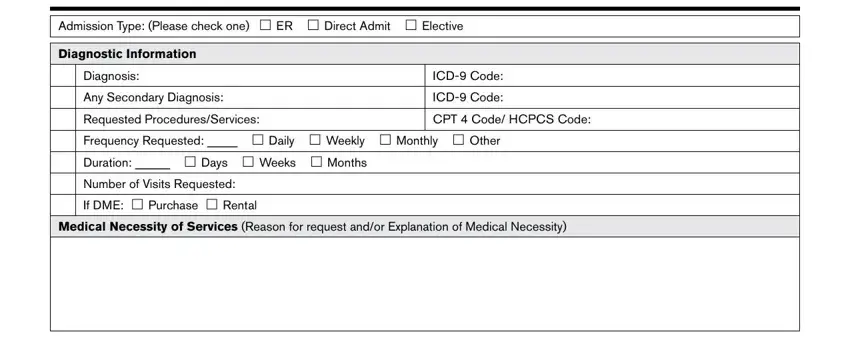
Put together the key particulars in the Admission Type Please check one, Diagnostic Information, Diagnosis, Any Secondary Diagnosis, ICD Code, ICD Code, Requested ProceduresServices, CPT Code HCPCS Code, and Medical Necessity of Services section.
Step 3: After you have selected the Done button, your document should be obtainable for export to any kind of gadget or email you specify.
Step 4: It may be more convenient to keep duplicates of the form. You can rest assured that we won't distribute or see your data.
