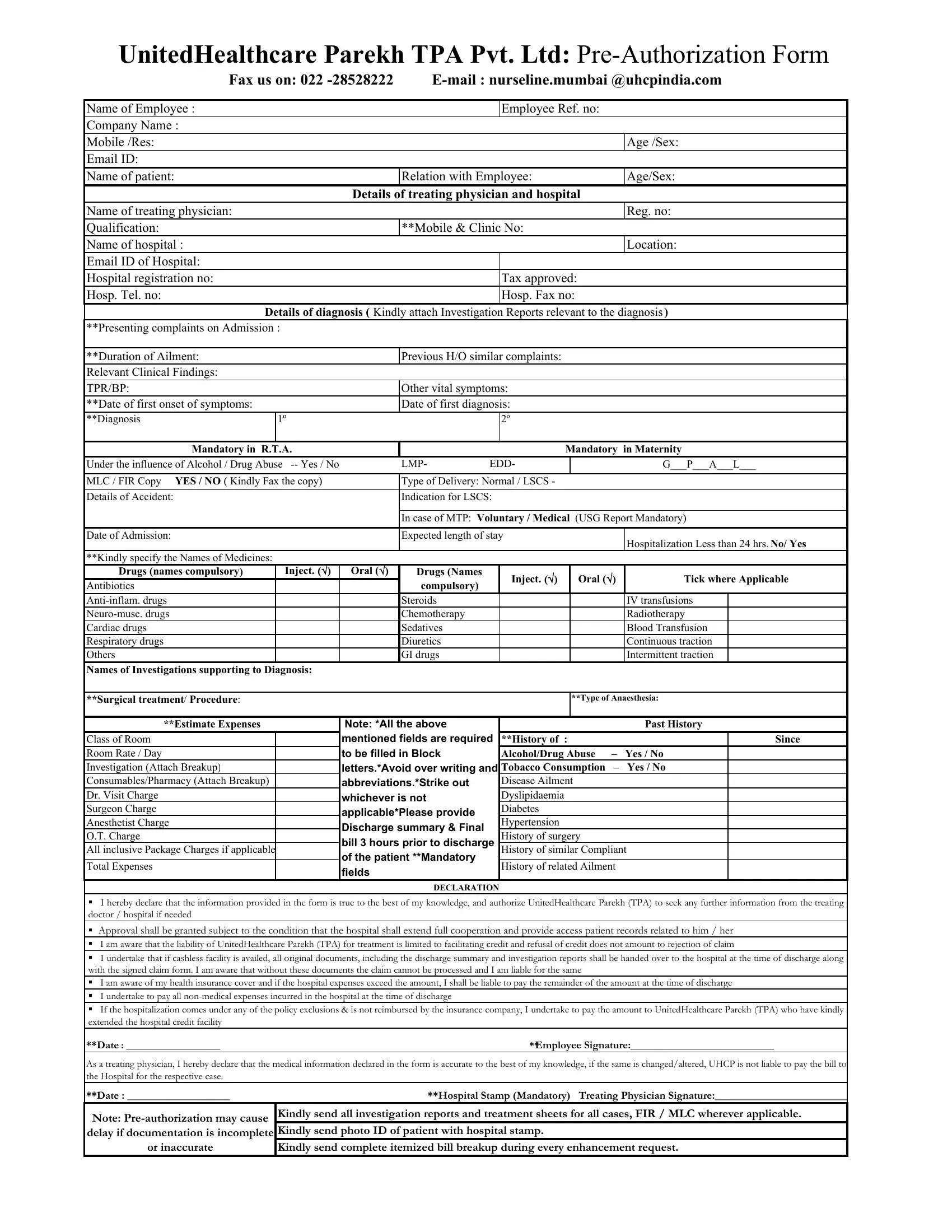
At the heart of healthcare management, especially when dealing with insurance claims and pre-authorizations, lies a complex network of procedural necessities aimed at ensuring both accuracy and compliance with policy stipulations. The United Healthcare Parekh Claim form serves as a critical instrument within this network, facilitating the seamless processing of insurance claims for employees needing medical services. This form encompasses a comprehensive range of details starting from basic identifiers such as the name of the employee, employee reference number, and company name, to more nuanced information including the patient's relation to the employee, details of the treating physician, and the hospital's credentials. It meticulously captures every aspect of the medical condition or incident leading to the claim, including diagnosis, treatment details, expected stay duration, and a declaration section for both the claimant and the treating physician, affirming the authenticity of the information provided. The form mandates the submission of investigation reports supporting the diagnosis, a detailed account of drugs and procedures employed, and a breakdown of the estimated expenses, covering the room charges and all inclusive package charges if applicable. Moreover, it underscores the conditions under which approval for claims might be granted or denied, highlighting the necessity for full cooperation from the hospital in providing access to patient records. By filling out this form, employees initiate the process toward availing themselves of the healthcare benefits as stipulated in their insurance coverage, hence underscoring the importance of accuracy and thoroughness in its completion.
| Question | Answer |
|---|---|
| Form Name | United Healthcare Parekh Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | united health parekh claim form, unitedhealthcare preauth form, united healthcare parekh preauth form download, united health care parekh claim form |
UnitedHealthcare Parekh TPA Pvt. Ltd:
Fax us on: 022 |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Name of Employee : |
|
|
|
|
|
Employee Ref. no: |
|
|
|
||
Company Name : |
|
|
|
|
|
|
|
|
|
|
|
Mobile /Res: |
|
|
|
|
|
|
|
|
|
Age /Sex: |
|
Email ID: |
|
|
|
|
|
|
|
|
|
|
|
Name of patient: |
|
|
|
Relation with Employee: |
|
|
|
Age/Sex: |
|||
|
|
|
Details of treating physician and hospital |
|
|
|
|||||
Name of treating physician: |
|
|
|
|
|
|
|
|
|
Reg. no: |
|
Qualification: |
|
|
|
**Mobile & Clinic No: |
|
|
|
|
|
||
Name of hospital : |
|
|
|
|
|
|
|
|
|
Location: |
|
Email ID of Hospital: |
|
|
|
|
|
|
|
|
|
|
|
Hospital registration no: |
|
|
|
|
|
Tax approved: |
|
|
|
||
Hosp. Tel. no: |
|
|
|
|
|
Hosp. Fax no: |
|
|
|
||
Details of diagnosis ( Kindly attach Investigation Reports relevant to the diagnosis) |
|||||||||||
**Presenting complaints on Admission : |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**Duration of Ailment: |
|
|
|
Previous H/O similar complaints: |
|
|
|
|
|
||
Relevant Clinical Findings: |
|
|
|
|
|
|
|
|
|
|
|
TPR/BP: |
|
|
|
Other vital symptoms: |
|
|
|
|
|
||
**Date of first onset of symptoms: |
|
|
|
Date of first diagnosis: |
|
|
|
|
|
||
**Diagnosis |
1º |
|
|
|
2º |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Mandatory in R.T.A. |
|
|
|
|
Mandatory in Maternity |
||||||
Under the influence of Alcohol / Drug Abuse |
|
LMP- |
EDD- |
|
|
|
G___P___A___L___ |
||||
|
|
|
|
|
|
|
|
|
|
||
MLC / FIR Copy YES / NO ( Kindly Fax the copy) |
|
Type of Delivery: Normal / LSCS - |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Details of Accident: |
|
|
|
Indication for LSCS: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
In case of MTP: Voluntary / Medical (USG Report Mandatory) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Date of Admission: |
|
|
|
Expected length of stay |
|
|
|
Hospitalization Less than 24 hrs. No/ Yes |
|||
|
|
|
|
|
|
|
|
|
|
||
**Kindly specify the Names of Medicines: |
|
|
|
|
|
|
|
|
|
|
|
Drugs (names compulsory) |
|
Inject. () |
Oral () |
Drugs (Names |
|
Inject. () |
|
Oral () |
Tick where Applicable |
||
Antibiotics |
|
|
|
compulsory) |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Steroids |
|
|
|
|
|
IV transfusions |
|
|
|
|
|
Chemotherapy |
|
|
|
|
|
Radiotherapy |
|
|
Cardiac drugs |
|
|
|
Sedatives |
|
|
|
|
|
Blood Transfusion |
|
Respiratory drugs |
|
|
|
Diuretics |
|
|
|
|
|
Continuous traction |
|
Others |
|
|
|
GI drugs |
|
|
|
|
|
Intermittent traction |
|
Names of Investigations supporting to Diagnosis: |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||
**Surgical treatment/ Procedure: |
|
|
|
|
|
|
|
**Type of Anaesthesia: |
|||
|
|
|
|
|
|
|
|
|
|
||
**Estimate Expenses |
|
|
Note: *All the above |
|
|
|
|
|
Past History |
||
Class of Room |
|
|
mentioned fields are required |
**History of |
: |
|
|
|
Since |
||
Room Rate / Day |
|
|
to be filled in Block |
|
Alcohol/Drug Abuse |
– |
Yes / No |
|
|||
Investigation (Attach Breakup) |
|
|
letters.*Avoid over writing and |
Tobacco Consumption |
– |
Yes / No |
|
||||
Consumables/Pharmacy (Attach Breakup) |
|
|
abbreviations.*Strike out |
|
Disease Ailment |
|
|
|
|||
Dr. Visit Charge |
|
|
whichever is not |
|
Dyslipidaemia |
|
|
|
|||
Surgeon Charge |
|
|
applicable*Please provide |
|
Diabetes |
|
|
|
|
|
|
Anesthetist Charge |
|
|
|
Hypertension |
|
|
|
|
|
||
|
|
Discharge summary & Final |
|
|
|
|
|
|
|||
O.T. Charge |
|
|
|
History of surgery |
|
|
|
||||
|
|
bill 3 hours prior to discharge |
|
|
|
||||||
All inclusive Package Charges if applicable |
|
|
History of similar Compliant |
|
|||||||
|
|
of the patient **Mandatory |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||
Total Expenses |
|
|
|
History of related Ailment |
|
|
|||||
|
|
fields |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DECLARATION |
|
|
|
|
|
|
|
I hereby declare that the information provided in the form is true to the best of my knowledge, and authorize UnitedHealthcare Parekh (TPA) to seek any further information from the treating doctor / hospital if needed
Approval shall be granted subject to the condition that the hospital shall extend full cooperation and provide access patient records related to him / her
I am aware that the liability of UnitedHealthcare Parekh (TPA) for treatment is limited to facilitating credit and refusal of credit does not amount to rejection of claim
I undertake that if cashless facility is availed, all original documents, including the discharge summary and investigation reports shall be handed over to the hospital at the time of discharge along with the signed claim form. I am aware that without these documents the claim cannot be processed and I am liable for the same
I am aware of my health insurance cover and if the hospital expenses exceed the amount, I shall be liable to pay the remainder of the amount at the time of discharge
I undertake to pay all
If the hospitalization comes under any of the policy exclusions & is not reimbursed by the insurance company, I undertake to pay the amount to UnitedHealthcare Parekh (TPA) who have kindly extended the hospital credit facility
**Date : ___________________**Employee Signature:_____________________________
As a treating physician, I hereby declare that the medical information declared in the form is accurate to the best of my knowledge, if the same is changed/altered, UHCP is not liable to pay the bill to the Hospital for the respective case.
**Date : ___________________ |
**Hospital Stamp (Mandatory) Treating Physician Signature:_________________________ |
Note: |
Kindly send all investigation reports and treatment sheets for all cases, FIR / MLC wherever applicable. |
delay if documentation is incomplete |
Kindly send photo ID of patient with hospital stamp. |
or inaccurate |
Kindly send complete itemized bill breakup during every enhancement request. |