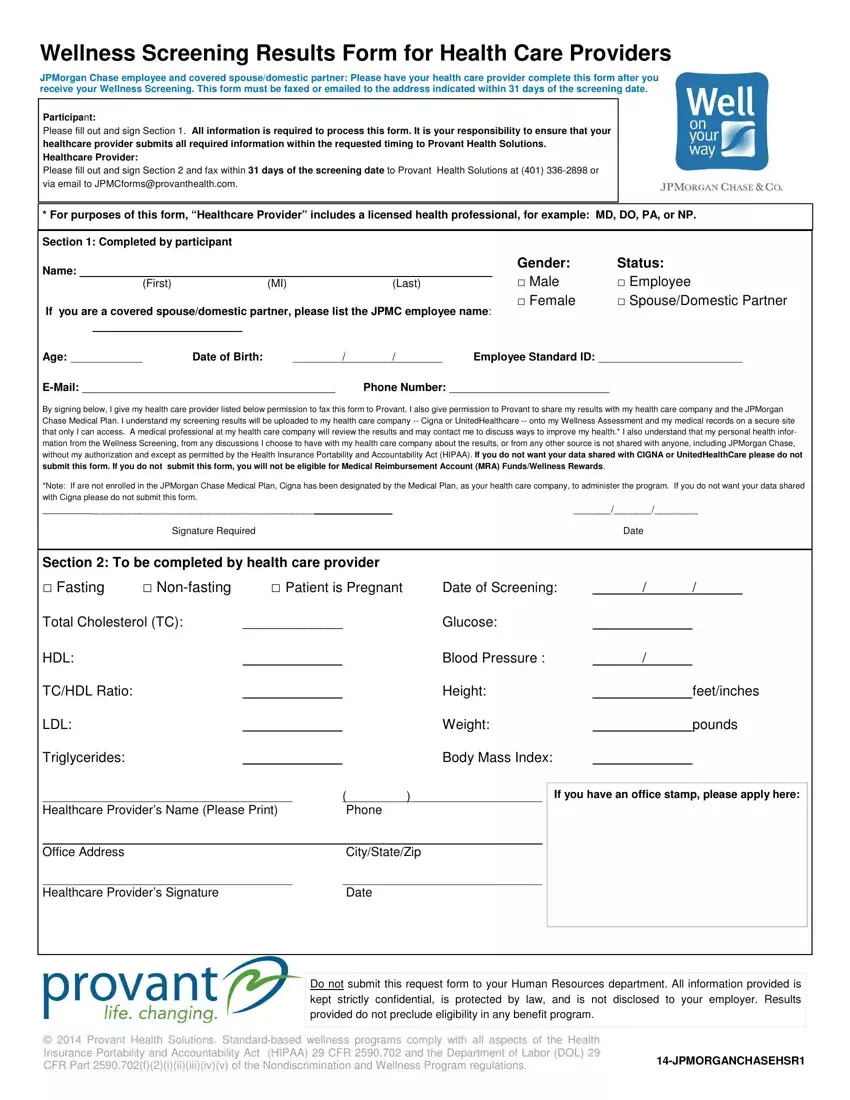
Wellness Screening Results Form for Health Care Providers
JPMorgan Chase employee and covered spouse/domestic partner: Please have your health care provider complete this form after you receive your Wellness Screening. This form must be faxed or emailed to the address indicated within 31 days of the screening date.
Participant:
Please fill out and sign Section 1. All information is required to process this form. It is your responsibility to ensure that your healthcare provider submits all required information within the requested timing to Provant Health Solutions.
Healthcare Provider:
Please fill out and sign Section 2 and fax within 31 days of the screening date to Provant Health Solutions at (401) 336-2898 or via email to JPMCforms@provanthealth.com.
* For purposes of this form, “Healthcare Provider” includes a licensed health professional, for example: MD, DO, PA, or NP.
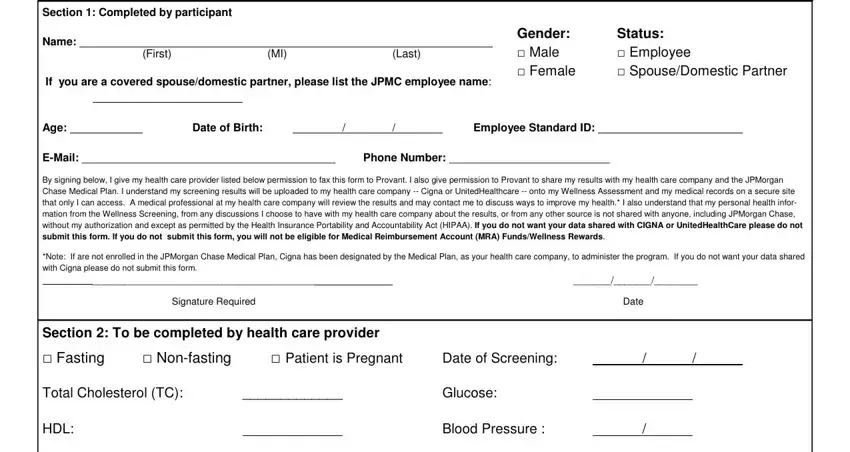
Section 1: Completed by participant
Name: |
|
|
Gender: |
Status: |
|
|
Male |
Employee |
|
(First) |
(MI) |
(Last) |
|
|
|
|
Female |
Spouse/Domestic Partner |
If you are a covered spouse/domestic partner, please list the JPMC employee name:
Age: |
|
Date of Birth: |
|
/ |
/ |
Employee Standard ID: |
|
E-Mail: _________________________________________ |
|
Phone Number: __________________________ |
By signing below, I give my health care provider listed below permission to fax this form to Provant. I also give permission to Provant to share my results with my health care company and the JPMorgan Chase Medical Plan. I understand my screening results will be uploaded to my health care company -- Cigna or UnitedHealthcare -- onto my Wellness Assessment and my medical records on a secure site that only I can access. A medical professional at my health care company will review the results and may contact me to discuss ways to improve my health.* I also understand that my personal health infor- mation from the Wellness Screening, from any discussions I choose to have with my health care company about the results, or from any other source is not shared with anyone, including JPMorgan Chase, without my authorization and except as permitted by the Health Insurance Portability and Accountability Act (HIPAA). If you do not want your data shared with CIGNA or UnitedHealthCare please do not
submit this form. If you do not submit this form, you will not be eligible for Medical Reimbursement Account (MRA) Funds/Wellness Rewards.
*Note: If are not enrolled in the JPMorgan Chase Medical Plan, Cigna has been designated by the Medical Plan, as your health care company, to administer the program. If you do not want your data shared with Cigna please do not submit this form.
|
_________________________________________ |
|
|
|
|
_______/_______/________ |
|
|
|
Signature Required |
|
|
Date |
|
|
Section 2: To be completed by health care provider |
|
|
|
|
|
Fasting |
Non-fasting |
Patient is Pregnant |
Date of Screening: |
/ |
/ |
|
Total Cholesterol (TC): |
_____________ |
|
Glucose: |
|
|
|
|
HDL: |
|
|
|
|
|
Blood Pressure : |
/ |
|
|
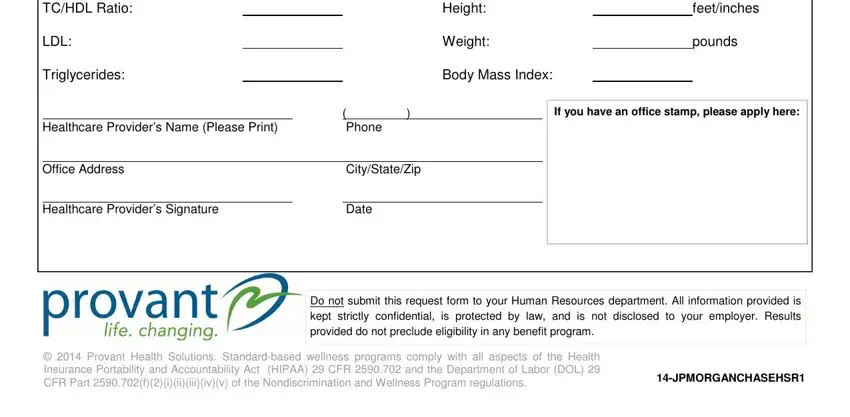
TC/HDL Ratio: |
|
|
|
|
|
Height: |
|
|
feet/inches |
LDL: |
|
|
|
|
|
Weight: |
|
|
pounds |
Triglycerides: |
|
|
|
|
|
Body Mass Index: |
|
|
|
|
|
( |
) |
If you have an office stamp, please apply here: |
Healthcare Provider’s Name (Please Print) |
|
Phone |
|
|
|
|
|
|
Office Address |
|
City/State/Zip |
|
|
|
|
|
|
Healthcare Provider’s Signature |
|
Date |
|
|
Do not submit this request form to your Human Resources department. All information provided is kept strictly confidential, is protected by law, and is not disclosed to your employer. Results provided do not preclude eligibility in any benefit program.
© 2014 Provant Health Solutions. Standard-based wellness programs comply with all aspects of the Health
|
Insurance Portability and Accountability Act (HIPAA) 29 CFR 2590.702 and the Department of Labor (DOL) 29 |
14-JPMORGANCHASEHSR1 |
|
CFR Part 2590.702(f)(2)(i)(ii)(iii)(iv)(v) of the Nondiscrimination and Wellness Program regulations. |
|
|