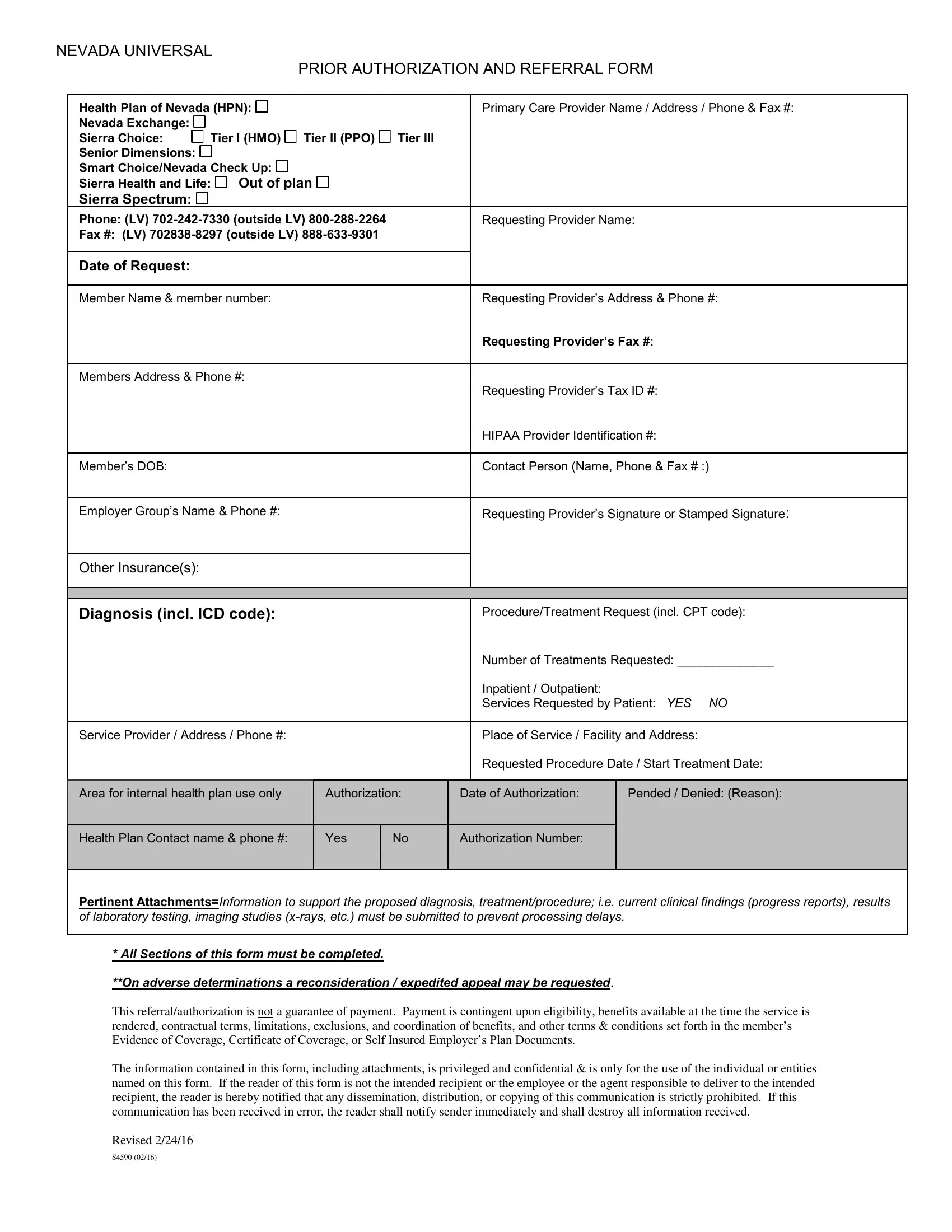
In the healthcare landscape of Nevada, the Universal Prior Authorization and Referral Form stands as a pivotal document streamlining the process of obtaining necessary medical referrals and prior authorizations. Crafted with meticulous detail, this form is utilized by various health plans including Health Plan of Nevada, Sierra Choice, and Senior Dimensions among others, catering to a wide spectrum of coverage tiers from HMOs to PPOs and beyond. This comprehensive tool is designed to facilitate a seamless communication pipeline between healthcare providers and insurance entities, ensuring that patients receive timely and efficient access to the medical services they need. By requiring detailed information such as the primary care provider's details, member identification, diagnosis and proposed treatment codes, and a thorough account of clinical findings, the form serves to expedite the decision-making process while maintaining a high standard of care. Furthermore, it outlines clear protocols for the submission of supporting documents, such as progress reports and laboratory test results, thereby minimizing potential delays in processing. Notably, the form also addresses the financial aspects of care, emphasizing that authorization does not guarantee payment but depends on a multitude of factors including eligibility, benefits available, and specific terms of coverage. Secure in its structure, the form ensures privacy and confidentiality in handling patient information, adhering strictly to HIPAA guidelines. A thoughtful feature allows for the request of reconsideration or expedited appeals in cases of adverse determinations, highlighting a commitment to fairness and patient advocacy. Revised last on February 24, 2016, this document encapsulates a critical effort in enhancing the efficiency and clarity of healthcare administration in Nevada.
| Question | Answer |
|---|---|
| Form Name | Universal Referral Form Nevada |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Universal Referral Prior Auth form referal sheet of anc form |
