
How to Fill Out the Compounding Universal Claim Form
Follow these steps to complete the form accurately. Having your insurance card, pharmacy receipt, and prescription label ready before you start will make the process faster.
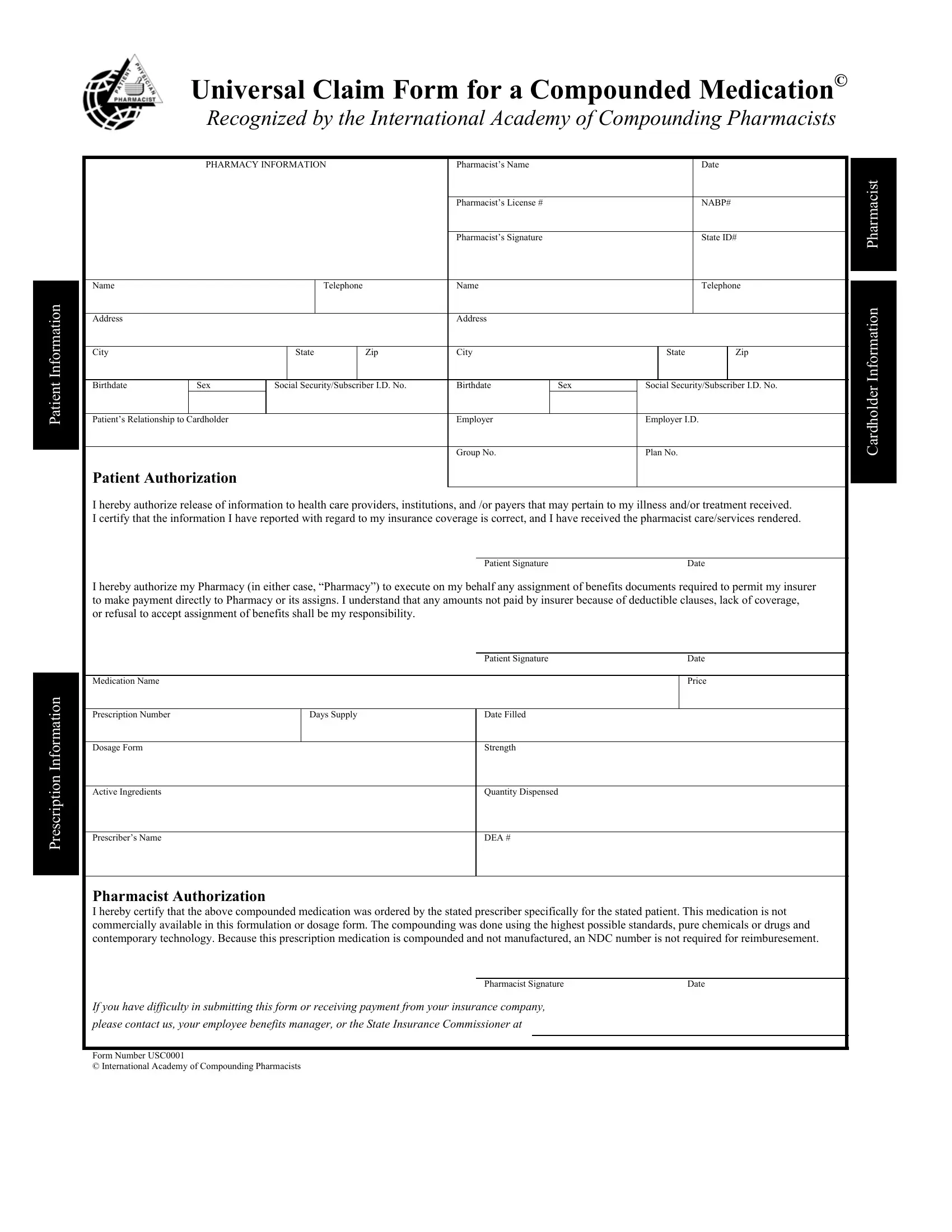
- Gather required documents - Collect your health insurance card, the paid pharmacy receipt, and a copy of the original compounded prescription. You will need the insurance member ID, group plan number, and the pharmacy's NCPDP provider number to complete the form.
- Enter patient information - Write your full legal name, date of birth, and mailing address exactly as they appear on your insurance records. Enter the health plan name and member ID from your insurance card. Any discrepancy with the insurer's files can delay processing.
- Record prescription details - Write the name of the compounded medication, the prescribed dosage and strength, the quantity the pharmacy dispensed, and the fill date. Include your prescribing physician's full name, phone number, and NPI number if shown on the prescription.
- Add pharmacy information - The compounding pharmacy fills in its name, address, NCPDP provider number, and the attending pharmacist's signature. Ask the pharmacy to complete these fields if your copy of the form is blank in this section.
- Sign the authorization section - Read the authorization statement before signing. Your signature and date allow the insurer to process the claim and to share information with the pharmacy as needed. Leaving this section blank will cause the insurer to reject the form.
- Attach supporting documents and submit - Include a copy of the prescription and the pharmacy receipt with the completed form. Mail the full package to the claims address printed on your insurance card. If your plan accepts online submissions, upload through the member portal and save the confirmation number.
Frequently Asked Questions
What is the Compounding Universal Claim Form?
The Compounding Universal Claim Form is a standardized document that patients use to request insurance reimbursement for compounded prescription medications. The International Academy of Compounding Pharmacists endorses this universal format to provide a consistent submission standard for compounding pharmacies and health insurers across the country.
Who needs to complete this form?
Patients who pay out of pocket for a compounded prescription and want reimbursement from their health plan must complete this form. In some cases, the compounding pharmacy assists with the pharmacy-specific sections and provides the required signatures before returning the form to the patient for submission.
How long does reimbursement take after I submit the form?
Processing times vary by insurer. Most commercial health plans review and respond to a complete claim form submission within 10 to 30 business days. Claims that are missing required information or documents may take longer. Call your insurer's member services line to verify receipt and track the status of your claim.
Can I fill out this claim form online?
Yes. You can fill out, edit, and download the Compounding Universal Claim Form online using FormsPal at no charge. The online tool lets you complete all required fields directly in your browser, then save the finished form as a PDF to print and mail to your insurer or upload through your plan's member portal.