
Through the online editor for PDFs by FormsPal, you're able to fill out or edit uson application form pdf right here and now. The editor is consistently upgraded by us, receiving awesome functions and growing to be better. It just takes a couple of basic steps:
Step 1: Access the PDF file inside our tool by clicking the "Get Form Button" above on this webpage.
Step 2: When you open the file editor, you will find the document made ready to be filled out. Besides filling out various blank fields, you may as well do several other things with the file, specifically adding any words, changing the original textual content, adding images, placing your signature to the form, and more.
To be able to fill out this PDF document, be sure you type in the required details in every single area:
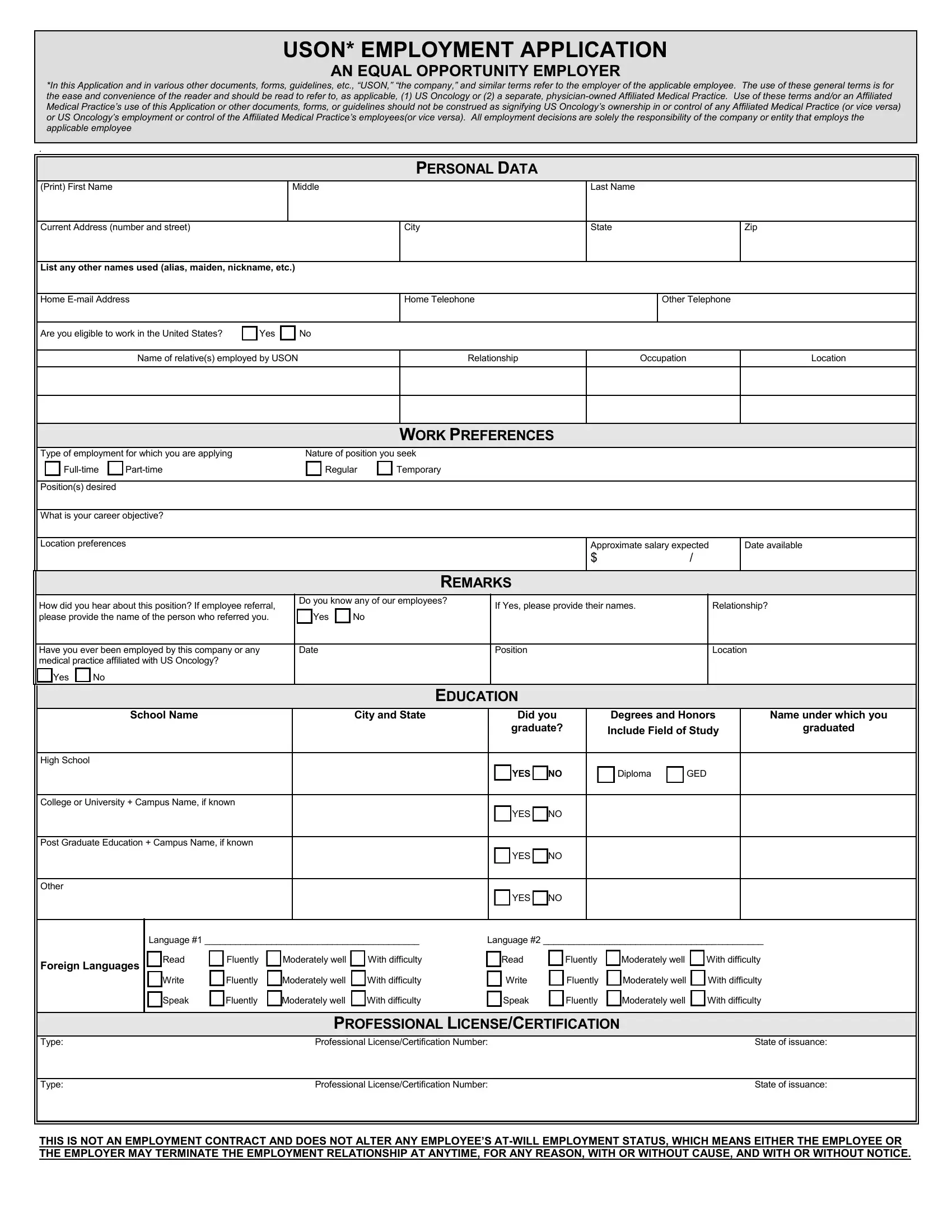
1. First of all, once completing the uson application form pdf, begin with the form section containing following fields:
2. Once your current task is complete, take the next step – fill out all of these fields - High School, College or University Campus Name, Post Graduate Education Campus, Other, Foreign Languages, YES NO Diploma GED, YES NO, YES NO, YES NO, Language Language, Read Fluently Moderately well, PROFESSIONAL LICENSECERTIFICATION, Type Professional, Type Professional, and THIS IS NOT AN EMPLOYMENT CONTRACT with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Within this step, have a look at Applicant Name, ADDITIONAL SKILLS, APPLICANT SHOULD NOTE ANY, Special Abilities Computer Skills, Branch of US Services, Nature of duties and any special, US MILITARY SERVICE, Date Entered, Date Discharged, Month, Year, Month, Year, From To, and LIST THE TWO MOST RECENT EMPLOYERS. Each one of these will have to be filled in with utmost awareness of detail.
Always be really careful while filling in Date Discharged and Special Abilities Computer Skills, since this is the part in which most people make a few mistakes.
4. Filling out From To, per, Name of Supervisor Telephone Number, Name used if different from, Reason for Leaving, Date, Company Name Street Address City, Month and Year, List TempStaffing Agency if that, Position, Ending SalaryWage, From To, per, Name of Supervisor Telephone Number, and Name used if different from is essential in the next stage - don't forget to don't rush and fill out every empty field!
5. As you come close to the final parts of your file, you'll find a few extra requirements that need to be satisfied. In particular, Name and Relationship, Company Name and Location City and, Telephone, Type of drivers license held, DRIVING RECORD, TO BE COMPLETED IF IT IS A JOB, Expiration Date, State of Issue, Have you ever had a drivers, Yes No, and If Yes please explain must be filled out.
Step 3: Go through all the information you have inserted in the blanks and click on the "Done" button. Make a 7-day free trial plan at FormsPal and get immediate access to uson application form pdf - download, email, or edit from your personal cabinet. FormsPal is dedicated to the privacy of our users; we ensure that all personal information processed by our editor stays secure.