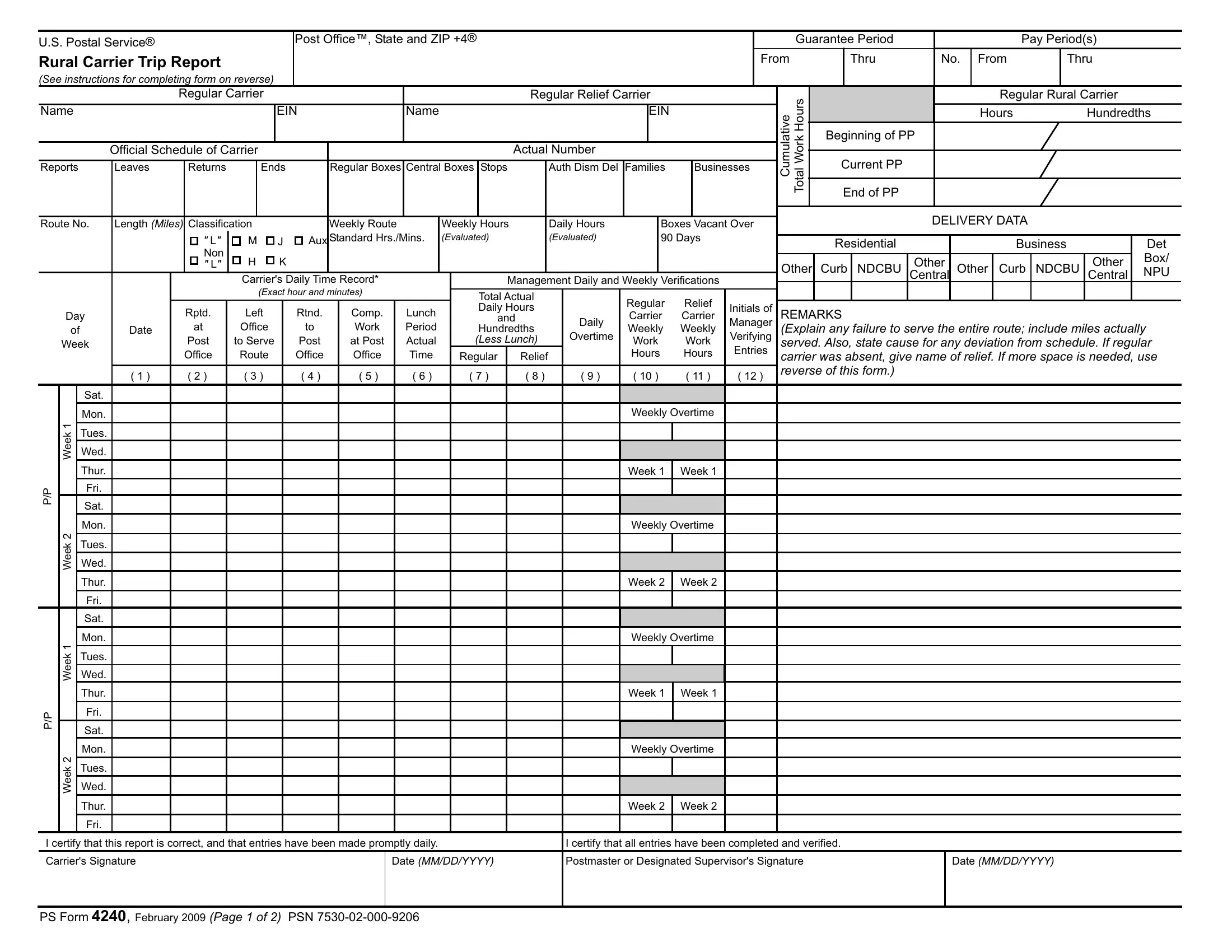
The USPS 4240 form, a crucial document for the U.S. Postal Service, plays a vital role in the operations of rural carriers, providing a structured method to report and verify their daily and weekly work hours, including regular and overtime hours, as well as specific delivery data. By detailing the start and end points of a carrier's route, the number of deliveries made—including regular, central, and curb boxes, and stops—it offers a comprehensive snapshot of a carrier's workload and efficiency. Management uses these reports for verifying work hours and ensuring rural carriers are compensated correctly, especially considering the fluctuations in daily deliveries and the need for adjustments due to unexpected events or route changes. Instructions on the form guide both the carriers in filling out their delivery data and supervisors in completing their verification processes, making it an essential tool for the accurate recording of operational metrics and, crucially, for the adjustment of carriers' compensation when route evaluations change. This systematic recording and review process, outlined in the form, underscores its importance in maintaining the efficiency and reliability of postal delivery services in rural areas.
| Question | Answer |
|---|---|
| Form Name | Usps Form 4240 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | postal form 4240, usps ps form 4240, ps form e4240, form ds 4240 |
U.S. Postal Service® |
|
|
Post Office™, State and ZIP +4® |
|
|
|
|
Guarantee Period |
|
Pay Period(s) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Rural Carrier Trip Report |
|
|
|
|
|
|
|
|
From |
|
Thru |
No. |
From |
Thru |
|
||
(See instructions for completing form on reverse) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Regular Carrier |
|
|
|
Regular Relief Carrier |
|
|
Total Work Hours |
|
|
Regular Rural Carrier |
|
||||
Name |
|
|
|
EIN |
|
Name |
|
|
EIN |
|
Cumulative |
|
|
Hours |
Hundredths |
||
|
|
|
|
|
|
|
|
|
|
|
Beginning of PP |
|
|
|
|||
|
Official Schedule of Carrier |
|
|
|
|
Actual Number |
|
|
|
|
|
|
|
||||
Reports |
Leaves |
Returns |
|
Ends |
|
Regular Boxes Central Boxes Stops |
Auth Dism Del |
Families |
Businesses |
Current PP |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
End of PP |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Route No. |
Length (Miles) Classification |
|
|
Weekly Route |
Weekly Hours |
Daily Hours |
Boxes Vacant Over |
|
|
|
DELIVERY DATA |
|
|
||||
|
|
|
|
|
|
|
|
|
|||||||||
|
|
" L" |
M |
J |
Aux |
Standard Hrs./Mins. |
(Evaluated) |
(Evaluated) |
90 Days |
|
|
Residential |
|
Business |
|
Det |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
Non |
H |
K |
|
|
|
|
|
|
|
|
|
Other |
|
Other |
Box/ |
|
|
" L" |
|
|
|
|
|
|
Other |
Curb NDCBU |
|
||||||
|
|
|
Carrier's Daily Time Record* |
Management Daily and Weekly Verifications |
Central Other Curb NDCBU Central |
NPU |
|||||||||||
|
|
|
|
|
|
(Exact hour and minutes) |
|
|
|
TotalActual |
|
Regular |
Relief |
|
|
|
|
||||
|
Day |
Rptd. |
Left |
Rtnd. |
Comp. |
|
Lunch |
Daily Hours |
|
Initials of |
|
REMARKS |
|
||||||||
|
|
and |
|
Daily |
Carrier |
Carrier |
Manager |
|
|
||||||||||||
|
of |
|
Date |
at |
Office |
to |
Work |
|
Period |
Hundredths |
Weekly |
Weekly |
|
(Explain any failure to serve the entire route; include miles actually |
|||||||
|
Week |
Post |
to Serve |
Post |
at Post |
|
Actual |
|
(Less Lunch) |
Overtime |
Work |
Work |
Verifying |
|
served.Also, state cause for any deviation from schedule. If regular |
||||||
|
|
|
|
|
Office |
Route |
Office |
Office |
|
Time |
Regular |
|
Relief |
|
Hours |
Hours |
Entries |
|
carrier was absent, give name of relief. If more space is needed, use |
||
|
|
|
( 1 ) |
( 2 ) |
( 3 ) |
( 4 ) |
( 5 ) |
|
( 6 ) |
|
( 7 ) |
|
( 8 ) |
( 9 ) |
( 10 ) |
( 11 ) |
( 12 ) |
|
reverse of this form.) |
|
|
|
|
|
Sat. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mon. |
|
|
|
|
|
|
|
|
|
|
|
Weekly Overtime |
|
|
|
|
||
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tues. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Wed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Thur. |
|
|
|
|
|
|
|
|
|
|
|
Week 1 |
Week 1 |
|
|
|
|
|
P/P |
|
|
Fri. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sat. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Mon. |
|
|
|
|
|
|
|
|
|
|
|
Weekly Overtime |
|
|
|
|
||
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tues. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Wed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Thur. |
|
|
|
|
|
|
|
|
|
|
|
Week 2 |
Week 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fri. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sat. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
Mon. |
|
|
|
|
|
|
|
|
|
|
|
Weekly Overtime |
|
|
|
|
||
|
Week |
|
Tues. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Thur. |
|
|
|
|
|
|
|
|
|
|
|
Week 1 |
Week 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P/P |
|
|
Fri. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sat. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2 |
|
Mon. |
|
|
|
|
|
|
|
|
|
|
|
Weekly Overtime |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Week |
|
Tues. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Thur. |
|
|
|
|
|
|
|
|
|
|
|
Week 2 |
Week 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fri. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that this report is correct, and that entries have been made promptly daily. |
|
|
|
I certify that all entries have been completed and verified. |
|
||||||||||||||||
Carrier's Signature |
|
|
|
|
Date (MM/DD/YYYY) |
|
Postmaster or Designated Supervisor's Signature |
Date (MM/DD/YYYY) |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
PS Form 4240, February 2009 (Page 1 of 2) |
PSN |
|
|
|
|
|
|
|
|
|
|
||||||||||
INSTRUCTIONS
All entries shall be in ink. Complete one copy and retain at Post Office™.
Postmaster or Designated Supervisor shall:
•Complete all information blocks on the upper portion of the form.
•Complete Columns
•See that the carrier makes appropriate entries for each delivery trip in columns
•Determine total actual daily workhours and minutes and, using USPS® Notice 30, Conversion Table, or facsimile, convert this time to hours and hundreths and enter the time in Columns
•Record the CUMULATIVE TOTALS for actual hours worked by the regular carrier for the
•Record daily overtime for all actual time worked in excess of 12 hours a day or 8 hours a day, whichever is appropriate (National Agreement). Authorized overtime hours worked during prescribed Christmas period shall be identified by circling the entry
in column 9.
•Record weekly overtime for all hours and hundreths worked in excess of 56 or 40 in a week, whichever is appropriate (National Agreement), in the open blocks in Columns 10 and 11.
•Enter A/L, S/L, etc., in Column 7 when the regular carrier is on annual leave, sick leave, etc., enter hours worked each day by the relief carrier in Column 8.
•Submit amended PS Form 4003 if unnecessary travel can be eliminated or when otherwise required.
•During the pay period, if a sufficient number of boxes are added to or subtracted from the route to trigger a change in the route's evaluation, adjust the carrier's compensation as required in Article 9 2.C.10.
•Close out the PS Form 4240 and begin a new sheet of the Guarantee Period.
Carrier Shall:
•Make daily entries in Columns
•If additional space is required for REMARKS, use the ADDITIONAL INFORMATION space below; precede remarks by date(s) where appropriate.
•Record information regarding the changes (increase or decrease) in the number of boxes, stops, families, official route miles, etc., in the space below as the changes occur.
Names of Post Offices Supplied by Locked Pouch:
1. |
4. |
7. |
2. |
5. |
8. |
3. |
6. |
9. |
|
|
|
Use this information to update "DELIVERY DATA" when the next PS Form 4240 is prepared.
|
|
Box #, Street Address, |
|
Residential |
|
|
Business |
|
|
|
|
|
|
|
|
||
|
Boxes/Stops |
Apt./Suite # and |
|
|
Other |
|
|
|
Date |
(+) or |
Other |
Curb NDCBU |
Other |
Curb NDCBU |
|||
Customer's Name |
Central |
|||||||
|
|
|
|
|
|
Other Central
Det
Box/
NPU
Additional Information:
PS Form 4240,February 2009 (Reverse)