It is simple to fill out forms making use of our PDF editor. Updating the va dbq forms pdf document is a breeze in the event you stick to these steps:
Step 1: Click the orange button "Get Form Here" on the following webpage.
Step 2: So, you're on the file editing page. You may add content, edit current data, highlight particular words or phrases, place crosses or checks, insert images, sign the document, erase unrequired fields, etc.
If you want to complete the va dbq forms pdf PDF, enter the details for all of the segments:
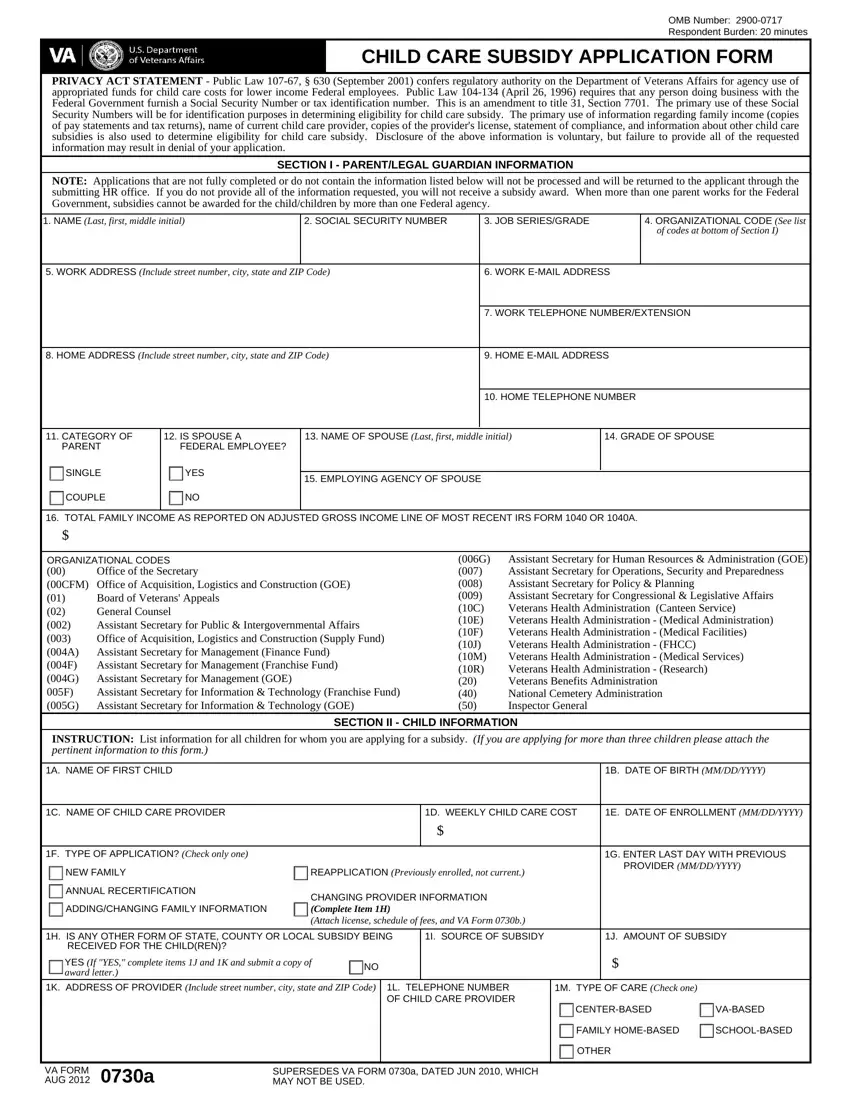
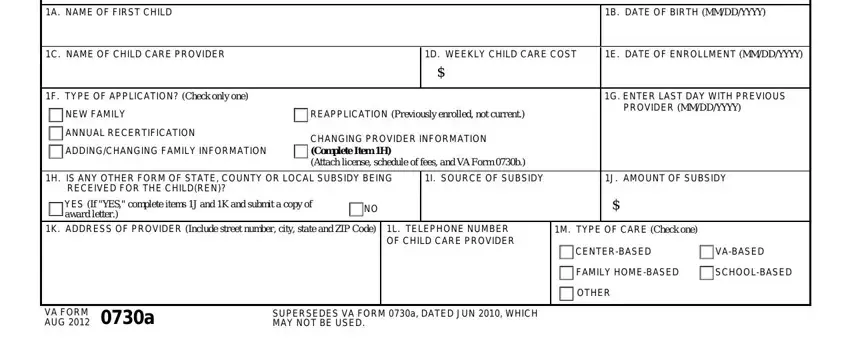
Enter the necessary details in the field A NAME OF FIRST CHILD, B DATE OF BIRTH MMDDYYYY, C NAME OF CHILD CARE PROVIDER, D WEEKLY CHILD CARE COST, E DATE OF ENROLLMENT MMDDYYYY, F TYPE OF APPLICATION Check only, NEW FAMILY, ANNUAL RECERTIFICATION, ADDINGCHANGING FAMILY INFORMATION, REAPPLICATION Previously enrolled, CHANGING PROVIDER INFORMATION, G ENTER LAST DAY WITH PREVIOUS, H IS ANY OTHER FORM OF STATE, I SOURCE OF SUBSIDY, and J AMOUNT OF SUBSIDY.
You need to point out the vital details in the A NAME OF SECOND CHILD, B DATE OF BIRTH MMDDYYYY, SECTION II CHILD INFORMATION, C NAME OF CHILD CARE PROVIDER, D WEEKLY CHILD CARE COST, E DATE OF ENROLLMENT MMDDYYYY, F TYPE OF APPLICATION Check only, NEW FAMILY, ANNUAL RECERTIFICATION, ADDINGCHANGING FAMILY INFORMATION, REAPPLICATION Previously enrolled, CHANGING PROVIDER INFORMATION, G ENTER LAST DAY WITH PREVIOUS, H IS ANY OTHER FORM OF STATE, and YES If YES complete items J and K section.
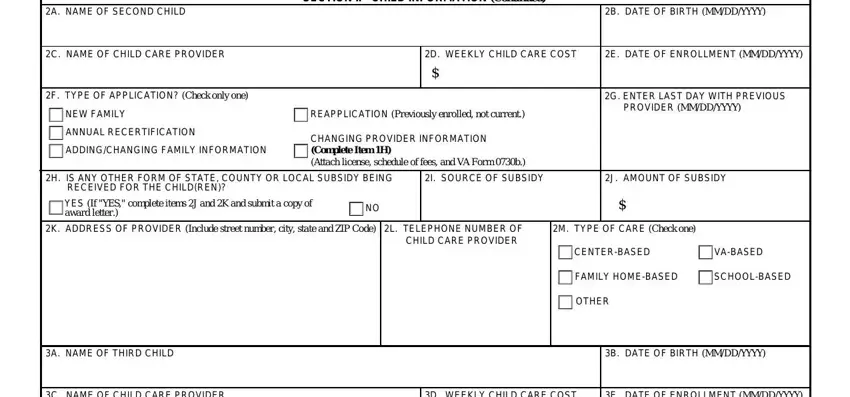
The area C NAME OF CHILD CARE PROVIDER, D WEEKLY CHILD CARE COST, E DATE OF ENROLLMENT MMDDYYYY, F TYPE OF APPLICATION Check only, NEW FAMILY, ANNUAL RECERTIFICATION, ADDINGCHANGING FAMILY INFORMATION, REAPPLICATION Previously enrolled, CHANGING PROVIDER INFORMATION, G ENTER LAST DAY WITH PREVIOUS, H IS ANY OTHER FORM OF STATE, YES If YES complete items J and K, I SOURCE OF SUBSIDY, J AMOUNT OF SUBSIDY, and K ADDRESS OF PROVIDER Include will be where to place all parties' rights and obligations.
End by checking the following sections and preparing them as needed: Signature, Date of signature MMDDYYYY, RESPONDENT BURDEN Public, and VA FORM a AUG PAGE.
Step 3: As you press the Done button, your ready form can be easily exported to each of your devices or to electronic mail given by you.
Step 4: Make sure you stay away from potential complications by making a minimum of a pair of copies of the document.
