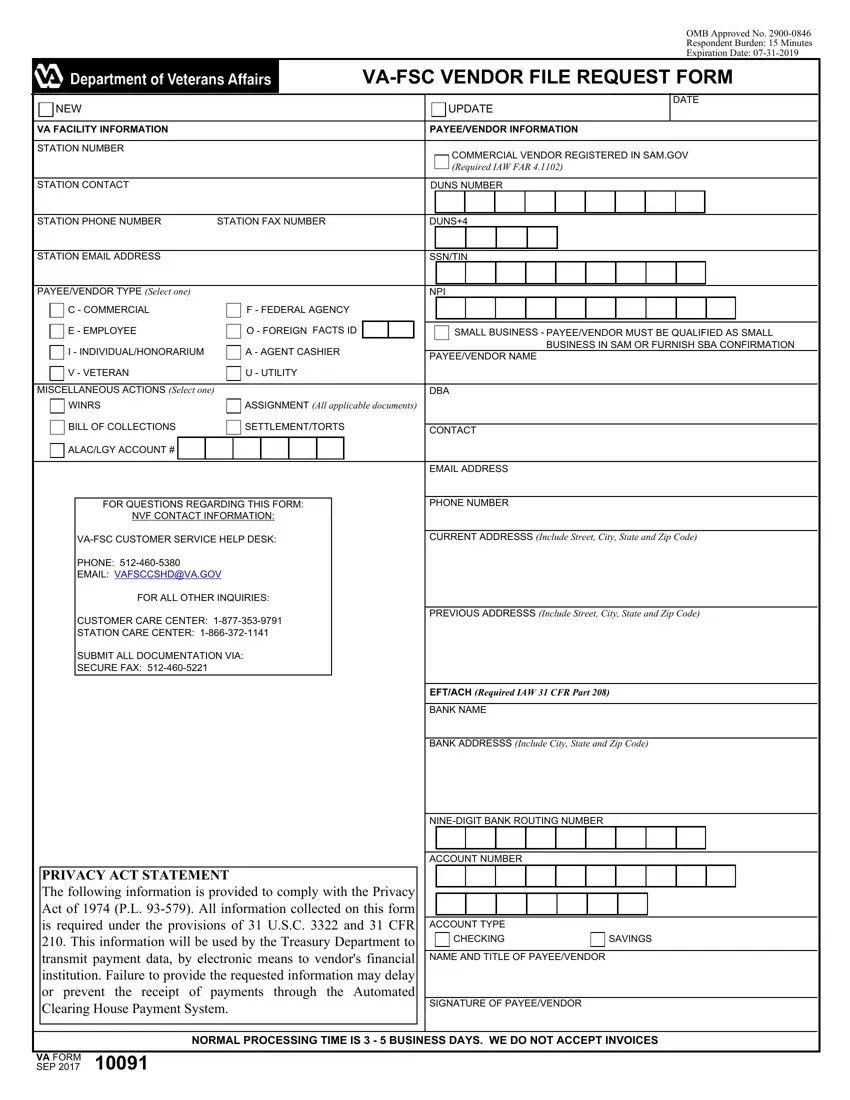
OMB Approved No. 2900-0846
Respondent Burden: 15 Minutes
Expiration Date: 07-31-2019
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VA-FSC VENDOR FILE REQUEST FORM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NEW |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UPDATE |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VA FACILITY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE/VENDOR INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATION NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMERCIAL VENDOR REGISTERED IN SAM.GOV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Required IAW FAR 4.1102) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATION CONTACT |
|
|
|
|
|
|
|
|
|
|
|
|
DUNS NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATION PHONE NUMBER |
STATION FAX NUMBER |
|
|
|
DUNS+4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATION EMAIL ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
SSN/TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE/VENDOR TYPE (Select one) |
|
|
|
|
|
|
|
|
|
|
|
|
NPI |
|
|
|
|
|
|
|
|
|
|
C - COMMERCIAL |
|
|
|
F - FEDERAL AGENCY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E - EMPLOYEE |
|
|
|
O - FOREIGN FACTS ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SMALL BUSINESS - PAYEE/VENDOR MUST BE QUALIFIED AS SMALL |
|
|
|
|
|
|
I - INDIVIDUAL/HONORARIUM |
|
|
|
A - AGENT CASHIER |
|
|
|
|
|
|
|
|
|
|
BUSINESS IN SAM OR FURNISH SBA CONFIRMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE/VENDOR NAME |
|
|
|
|
|
|
|
|
|
|
V - VETERAN |
|
|
|
U - UTILITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISCELLANEOUS ACTIONS (Select one) |
|
|
|
|
|
|
|
|
|
|
|
|
DBA |
|
|
|
|
|
|
|
|
|
|
WINRS |
|
|
|
ASSIGNMENT (All applicable documents) |
|
|
|
|
|
|
|
|
|
|
BILL OF COLLECTIONS |
|
|
|
SETTLEMENT/TORTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTACT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ALAC/LGY ACCOUNT # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMAIL ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
FOR QUESTIONS REGARDING THIS FORM: |
|
|
|
|
|
|
|
|
|
|
|
|
|
NVF CONTACT INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VA-FSC CUSTOMER SERVICE HELP DESK: |
|
|
|
|
|
CURRENT ADDRESSS (Include Street, City, State and Zip Code) |
|
|
|
|
|
|
|
PHONE: 512-460-5380 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMAIL: VAFSCCSHD@VA.GOV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR ALL OTHER INQUIRIES: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CUSTOMER CARE CENTER: 1-877-353-9791 |
|
|
|
|
|
PREVIOUS ADDRESSS (Include Street, City, State and Zip Code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATION CARE CENTER: 1-866-372-1141 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUBMIT ALL DOCUMENTATION VIA: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECURE FAX: 512-460-5221 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFT/ACH (Required IAW 31 CFR Part 208) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BANK NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BANK ADDRESSS (Include City, State and Zip Code) |
|
|
|
|
|
|
NINE-DIGIT BANK ROUTING NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCOUNT NUMBER |
|
|
|
|
|
|
PRIVACY ACT STATEMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The following information is provided to comply with the Privacy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Act of 1974 (P.L. 93-579). All information collected on this form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
is required under the provisions of 31 U.S.C. 3322 and 31 CFR |
|
ACCOUNT TYPE |
|
|
|
|
|
|
210. This information will be used by the Treasury Department to |
|
|
|
CHECKING |
|
|
SAVINGS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
transmit payment data, by electronic means to vendor's financial |
|
NAME AND TITLE OF PAYEE/VENDOR |
|
|
|
|
|
|
institution. Failure to provide the requested information may delay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or prevent the receipt of payments through the Automated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Clearing House Payment System. |
|
SIGNATURE OF PAYEE/VENDOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NORMAL PROCESSING TIME IS 3 - 5 BUSINESS DAYS. WE DO NOT ACCEPT INVOICES
Instructions for FMS Vendor File Request Form
1.NEW box option - Check box if you are a new vendor not in the FMS system.
2.UPDATE box option - Check box if you are an existing vendor in the FMS system.
VA Facility Information
3.Station # - This portion pertains to the VA Station submitting this form, provide your station 3 digit station number. FOR STATION USE
ONLY
4.Station Contact Name - VA Station employee. FOR STATION USE ONLY
5.Station Phone - VA Station employee direct number. FOR STATION USE ONLY
6.Station Fax Number - VA Station fax number. FOR STATION USE ONLY
7.Station Email - VA Station employee work email address. FOR STATION USE ONLY
Payee/Vendor Type - Check the appropriate Payee/Vendor Type box. REQUIRED
Miscellaneous Actions - Check the appropriate Payee/Vendor Type box, some additional documentation required.
OPTIONAL
·ALAC Vendors - USE ONLY IF ALAC include the 6 digit account number
·Assignment of Claims- USE ONLY IF ASSIGNMENT include Notice of Assignment & Instrument of Assignment
·Federal Vendors- USE ONLY IF FEDERAL AGENCY include the 2 digit Facts
·Foreign Vendors- USE ONLY FOR FOREIGN COUNTRY include W8Ben with foreign identification number
Payee/Vendor Information
8.Commercial Vendor Registered in SAM.gov - If you are registered in System of Awards Management & have a DUNS number check this box. OPTIONAL
9.DUNS # - Data Universal Numbering System (DUNS) is a unique 9-digit number that is administered by Dun and Bradstreet (D&B)
OPTIONAL
10.DUNS+4 - If you have more than one EFT account number for the same DUNS number and same physical location as defined by the DUNS address complete this section. OPTIONAL
11.SSN/TIN - The Social Security Number (SSN) is the nine-digit number. The Tax Identification Number (TIN) is the nine-digit number which is either an Employer Identification Number (EIN); complete this section with SSN, TIN, EIN or ITIN. REQUIRED
12.NPI - A standard 10 digit unique identifiers for health care providers, complete this section if applicable. OPTIONAL
13.Small Business - Check box if applicable OPTIONAL
14.Vendor Name - Provide legal name as it is on file with the IRS REQUIRED
15.DBA - Doing Business As name complete if applicable OPTIONAL
16.Contact - Name of Point of Contact if additional information is required OPTIONAL
17.Email - Point of Contact email address OPTIONAL
18.Phone - Point of Contact phone number OPTIONAL
19.Current Address - Provide your most current address, city, state & zip code REQUIRED
20.Previous Address - Provide previous address, city, state and zip code REQUIRED FOR ADDRESS CHANGES
EFT/ACH (REQUIRED IAW 31CFR Part 208)
21.US. Bank Name - provide financial institution name city, state & zip code. REQUIRED
22.US. Nine-Digit Bank Routing Number - Provide 9 digit routing number from check ( DO NOT use Deposit slip routing number)
REQUIRED
23.US. Account # - Provide bank account number maximum 17 digits REQUIRED
24.Account Type - Check appropriate box that is associated with account number provide above REQUIRED
25.Name & Title of Payee/Vendor - REQUIRED
26.Signature of Payee/Vendor - REQUIRED
Please fax the completed form to 512-460-5221 for processing.
PRIVACY ACT NOTICE: The following information is provided to comply with the Privacy Act of 1974 (P.L. 93-579). All information collected on this form is required under the provisions of 31 U.S.C. 3322 and 31 CFR 210. This information will be used by the Treasury Department to transmit payment data, by electronic means to vendor's financial institution. Failure to provide the requested information may delay or prevent the receipt of payments through the Automated Clearing House Payment System.
RESPONDENT BURDEN: The Nationwide Vendor File Division needs this information to establish, modify/change your VA Vendor Record.
31 U.S.C. 3322 and 31 CFR 210, allow us to ask for this information. We estimate that you will need an average of 15 minutes to review the instructions, find the information, and complete this form. VA cannot conduct or sponsor a collection of information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not displayed. Valid OMB control numbers can be located on the OMB Internet Page at www.reginfo.gov/public/do/PRAMain.