
change direct appropriate get can be completed online effortlessly. Just use FormsPal PDF editor to finish the job without delay. Our editor is constantly evolving to deliver the very best user experience achievable, and that's because of our resolve for constant enhancement and listening closely to testimonials. With just a few easy steps, you are able to start your PDF editing:
Step 1: Just click the "Get Form Button" above on this webpage to start up our pdf file editor. There you'll find all that is needed to work with your document.
Step 2: After you launch the PDF editor, you will see the document made ready to be completed. Besides filling in different fields, you might also do various other things with the file, that is writing any textual content, editing the initial textual content, inserting illustrations or photos, placing your signature to the document, and more.
This document requires specific information; in order to ensure correctness, make sure you bear in mind the subsequent tips:
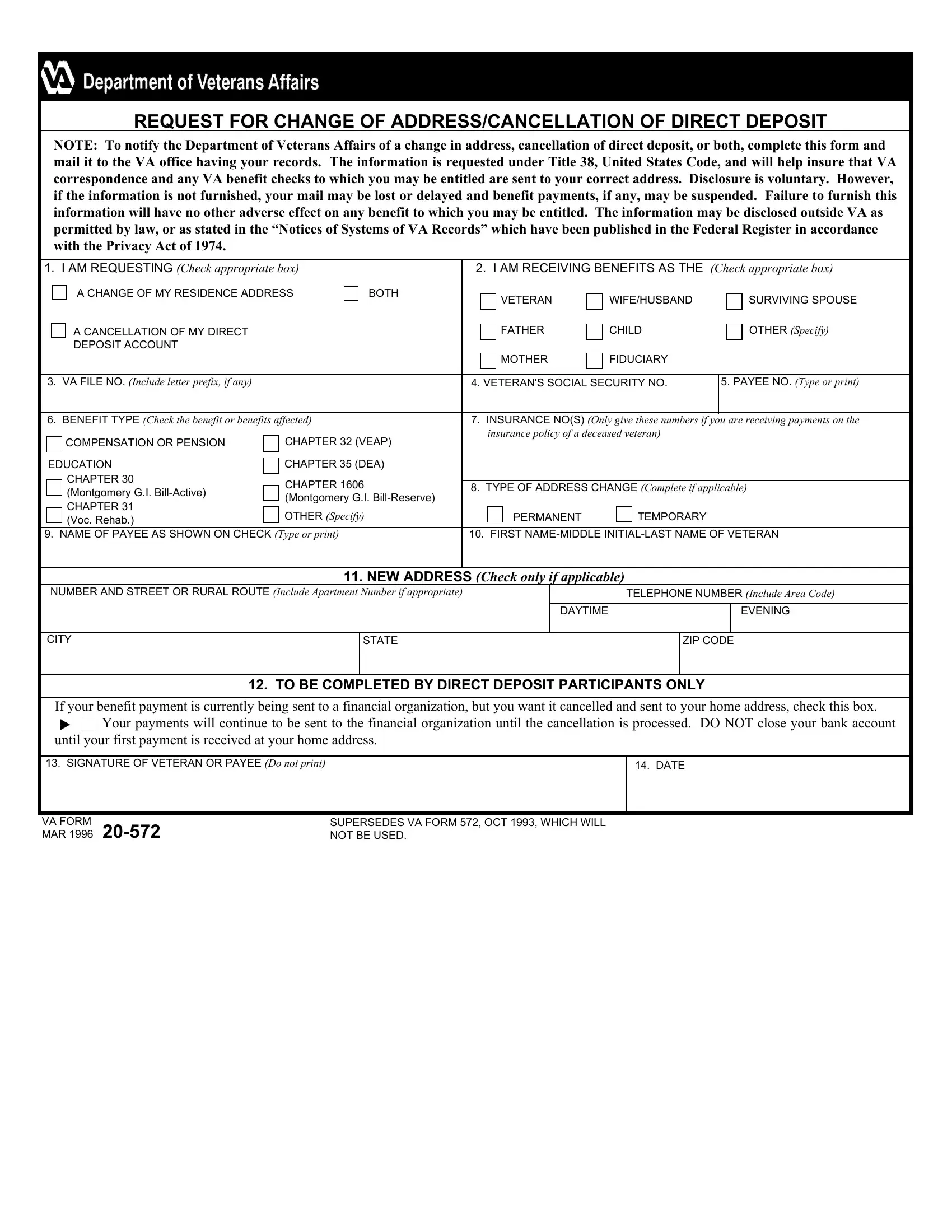
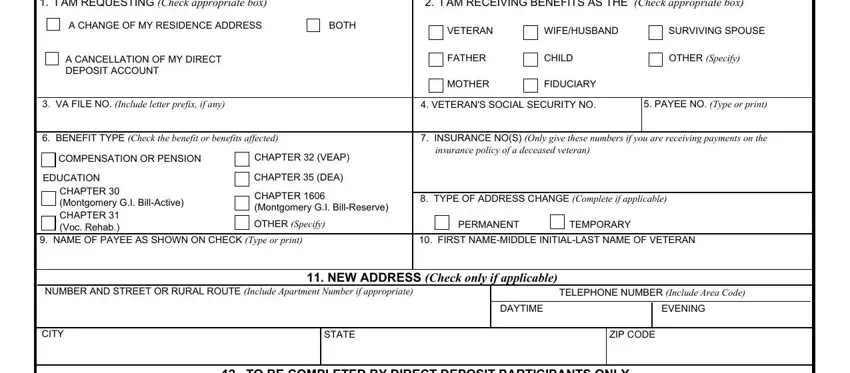
1. It is recommended to complete the change direct appropriate get accurately, therefore be attentive while working with the sections that contain these fields:
2. The subsequent part is to fill in these blank fields: If your benefit payment is, SIGNATURE OF VETERAN OR PAYEE Do, DATE, VA FORM MAR, and SUPERSEDES VA FORM OCT WHICH.
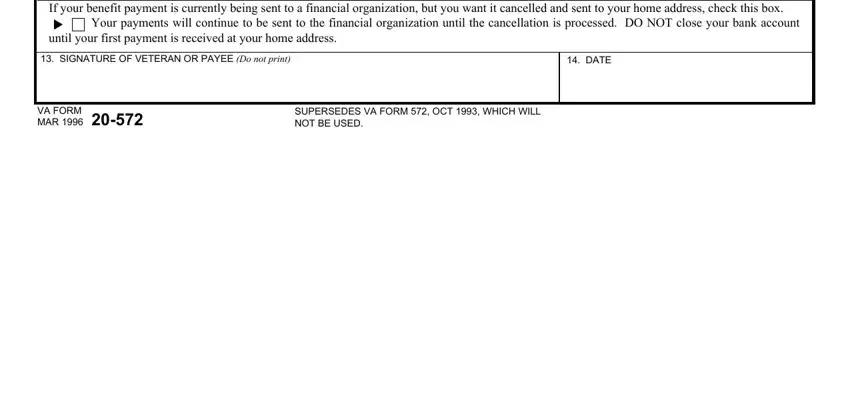
When it comes to SUPERSEDES VA FORM OCT WHICH and If your benefit payment is, make sure you take a second look in this current part. Both these are definitely the key fields in this page.
Step 3: Revise everything you have typed into the blank fields and then press the "Done" button. Sign up with us right now and instantly gain access to change direct appropriate get, ready for downloading. Each edit you make is conveniently saved , helping you to modify the file at a later time if required. When using FormsPal, you can easily complete forms without having to be concerned about personal information leaks or entries being shared. Our secure system helps to ensure that your private data is stored safely.