
Handling PDF documents online is simple using our PDF tool. You can fill in form 0516 here in a matter of minutes. To have our editor on the leading edge of practicality, we work to implement user-driven features and improvements on a regular basis. We're always thankful for any feedback - assist us with reshaping the way you work with PDF forms. Getting underway is easy! All that you should do is follow these basic steps directly below:
Step 1: First of all, access the tool by clicking the "Get Form Button" at the top of this page.
Step 2: The tool enables you to work with PDF files in various ways. Transform it with personalized text, correct original content, and put in a signature - all doable in no time!
This PDF form requires particular data to be filled out, therefore be sure to take your time to type in precisely what is expected:
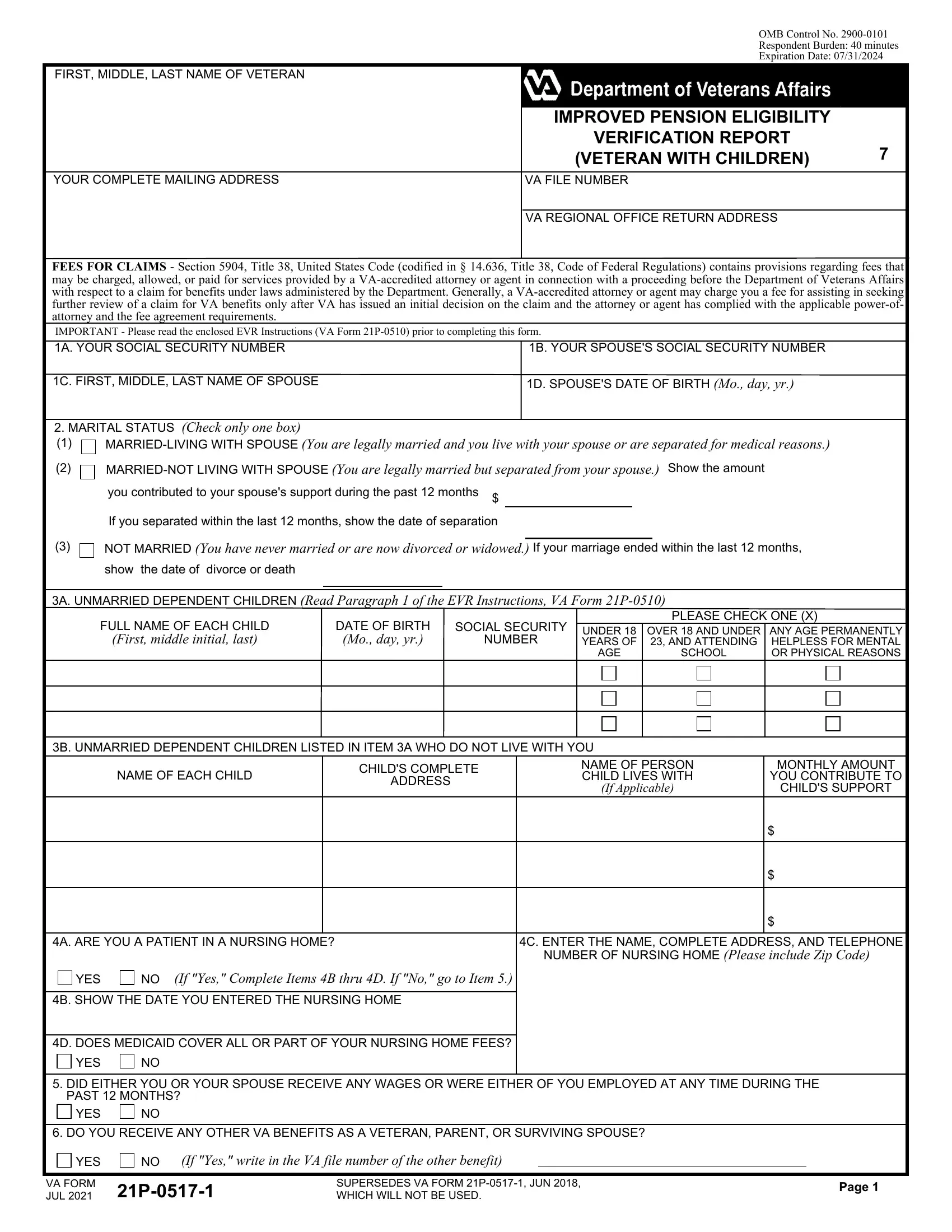
1. For starters, when filling out the form 0516, start with the area that includes the following blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - NOT MARRIED You have never married, If your marriage ended within the, show the date of divorce or death, A UNMARRIED DEPENDENT CHILDREN, FULL NAME OF EACH CHILD, First middle initial last, DATE OF BIRTH, Mo day yr, SOCIAL SECURITY, NUMBER, PLEASE CHECK ONE X, UNDER YEARS OF, OVER AND UNDER AND ATTENDING, AGE, and SCHOOL with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this step, examine C ENTER THE NAME COMPLETE ADDRESS, YES, If Yes Complete Items B thru D If, B SHOW THE DATE YOU ENTERED THE, D DOES MEDICAID COVER ALL OR PART, YES, DID EITHER YOU OR YOUR SPOUSE, YES, DO YOU RECEIVE ANY OTHER VA, YES, If Yes write in the VA file number, VA FORM JUL, SUPERSEDES VA FORM P JUN WHICH, and Page. Each one of these are required to be taken care of with greatest precision.
4. This next section requires some additional information. Ensure you complete all the necessary fields - GROSS MONTHLY AMOUNTS If no income, A MONTHLY INCOME Read Paragraphs, SOURCE, VETERAN, SPOUSE, SOCIAL SECURITY, U S CIVIL SERVICE, U S RAILROAD RETIREMENT, BLACK LUNG BENEFITS, MILITARY RETIREMENT, OTHER Show Source, OTHER Show Source, OTHER Show Source, CHILD, and NOTE Report annual income for the - to proceed further in your process!
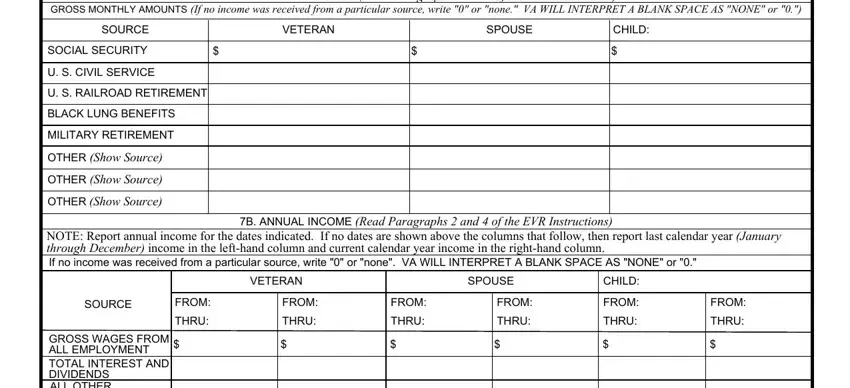
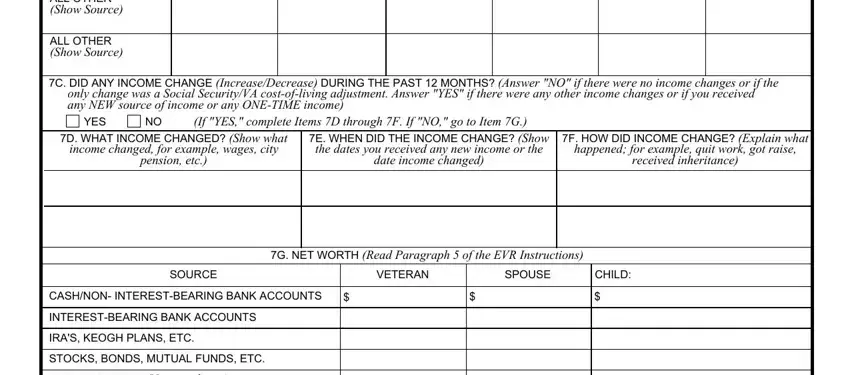
5. Finally, the following last portion is precisely what you'll have to finish prior to using the PDF. The blanks under consideration include the following: GROSS WAGES FROM ALL EMPLOYMENT, ALL OTHER Show Source, C DID ANY INCOME CHANGE, YES, If YES complete Items D through F, D WHAT INCOME CHANGED Show what, income changed for example wages, pension etc, E WHEN DID THE INCOME CHANGE Show, the dates you received any new, date income changed, F HOW DID INCOME CHANGE Explain, happened for example quit work got, received inheritance, and G NET WORTH Read Paragraph of the.
When it comes to D WHAT INCOME CHANGED Show what and GROSS WAGES FROM ALL EMPLOYMENT, make sure you get them right in this section. Those two could be the most important fields in this PDF.
Step 3: Revise everything you've entered into the form fields and then click the "Done" button. Get your form 0516 when you register here for a 7-day free trial. Easily get access to the form within your personal account page, together with any modifications and changes all kept! We do not sell or share any details that you provide whenever completing forms at our website.