
You are able to prepare SSN instantly by using our PDFinity® online PDF tool. To maintain our editor on the cutting edge of practicality, we work to put into operation user-oriented capabilities and enhancements on a regular basis. We're always looking for suggestions - help us with revolutionizing how we work with PDF docs. This is what you'll need to do to start:
Step 1: Open the form in our editor by clicking the "Get Form Button" above on this webpage.
Step 2: With our advanced PDF editing tool, you could accomplish more than just complete blanks. Express yourself and make your forms look high-quality with customized textual content added in, or adjust the file's original input to perfection - all that comes with the capability to incorporate your own photos and sign the file off.
Pay close attention while filling out this pdf. Ensure that all necessary fields are completed properly.
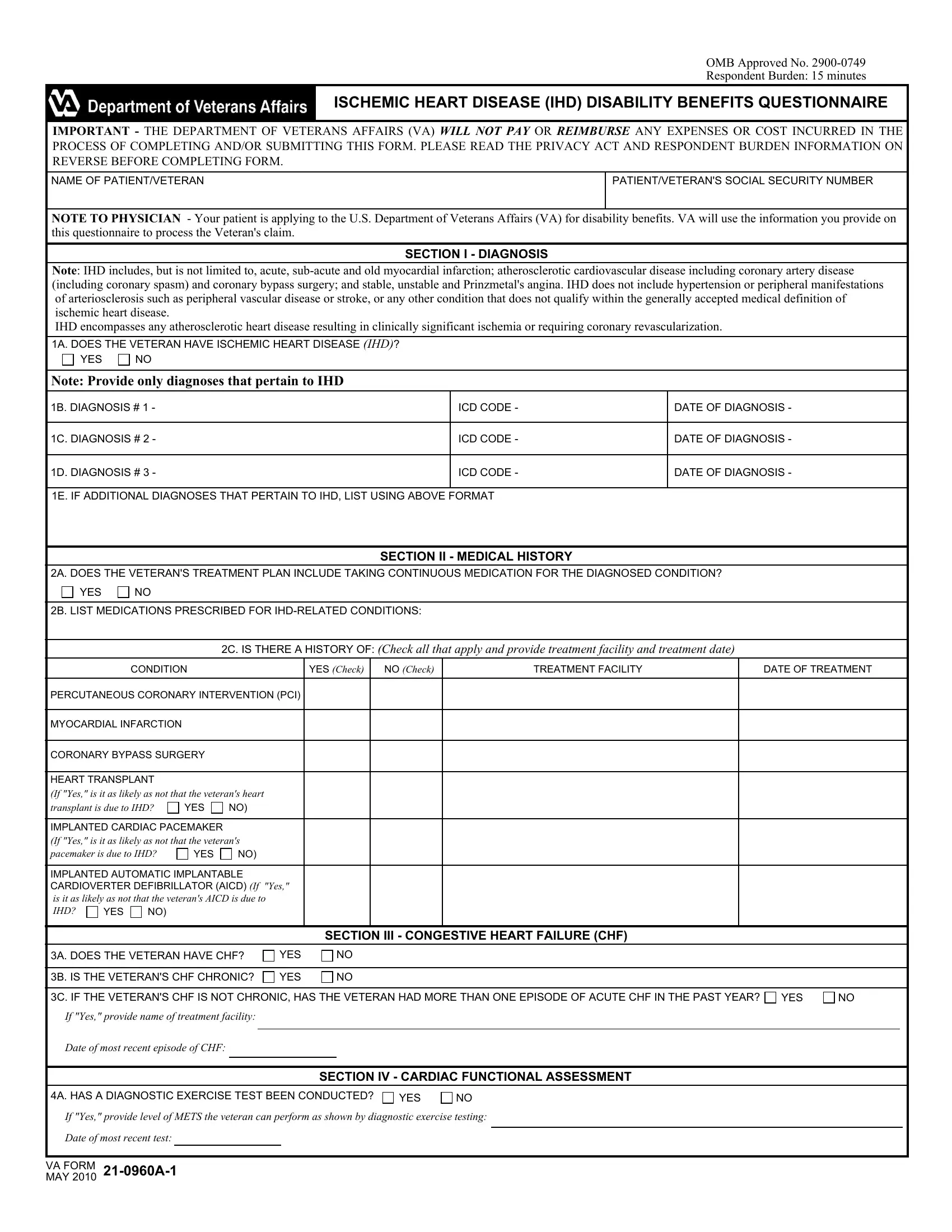
1. Fill out the SSN with a group of essential blanks. Note all of the necessary information and make sure nothing is forgotten!
2. Given that the previous array of fields is done, you're ready to insert the essential particulars in B LIST MEDICATIONS PRESCRIBED FOR, C IS THERE A HISTORY OF Check all, CONDITION, YES Check, NO Check, TREATMENT FACILITY, DATE OF TREATMENT, PERCUTANEOUS CORONARY INTERVENTION, MYOCARDIAL INFARCTION, CORONARY BYPASS SURGERY, HEART TRANSPLANT, If Yes is it as likely as not that, transplant is due to IHD, YES, and IMPLANTED CARDIAC PACEMAKER If Yes allowing you to proceed to the 3rd stage.

It is possible to make errors while completing your TREATMENT FACILITY, for that reason you'll want to go through it again before you'll submit it.
3. In this particular step, take a look at A HAS A DIAGNOSTIC EXERCISE TEST, YES, If Yes provide level of METS the, Date of most recent test, and VA FORM MAY A. Every one of these need to be taken care of with greatest accuracy.

4. Filling in Lowest level of activity at which, DYSPNEA, FATIGUE, ANGINA, DIZZINESS, SYNCOPE, This METs Level has been found to, METs This METs level has been, METs This METs level has been, METs This METs level has been, METs This METs level has been, Veteran denies experiencing above, NOTE Determination of cardiac, SECTION V DIAGNOSTIC TESTING, and A IS THERE EVIDENCE OF CARDIAC is vital in this fourth step - you should definitely invest some time and take a close look at each and every field!
5. The very last section to conclude this form is pivotal. You'll want to fill out the appropriate blank fields, for example DOES THE VETERANS IHD IMPACT THE, YES, NO If Yes describe impact, REMARKS If any, CERTIFICATION To the best of my, SECTION VII PHYSICIANS, A PHYSICIANS SIGNATURE, B PHYSICIANS PRINTED NAME, C DATE SIGNED, D PHYSICIANS PHONE NUMBER, E PHYSICIANS MEDICAL LICENSE NUMBER, F PHYSICIANS ADDRESS, NOTE VA may obtain additional, IMPORTANT Physician please fax, and VA Regional Office FAX No, before using the pdf. Neglecting to do so may end up in an incomplete and potentially nonvalid document!
Step 3: Reread the information you've entered into the blanks and then click on the "Done" button. Join FormsPal today and easily use SSN, prepared for download. Each change made is handily kept , meaning you can modify the pdf at a later stage as needed. FormsPal is dedicated to the privacy of our users; we ensure that all information handled by our system remains secure.