
Handling PDF documents online is definitely surprisingly easy with our PDF tool. Anyone can fill out 2012 here effortlessly. The tool is constantly upgraded by our team, receiving additional features and becoming better. In case you are looking to get started, here's what it requires:
Step 1: First, access the pdf editor by clicking the "Get Form Button" at the top of this page.
Step 2: The editor lets you change your PDF form in many different ways. Transform it by including personalized text, adjust existing content, and add a signature - all at your convenience!
As for the blank fields of this particular PDF, here's what you should do:
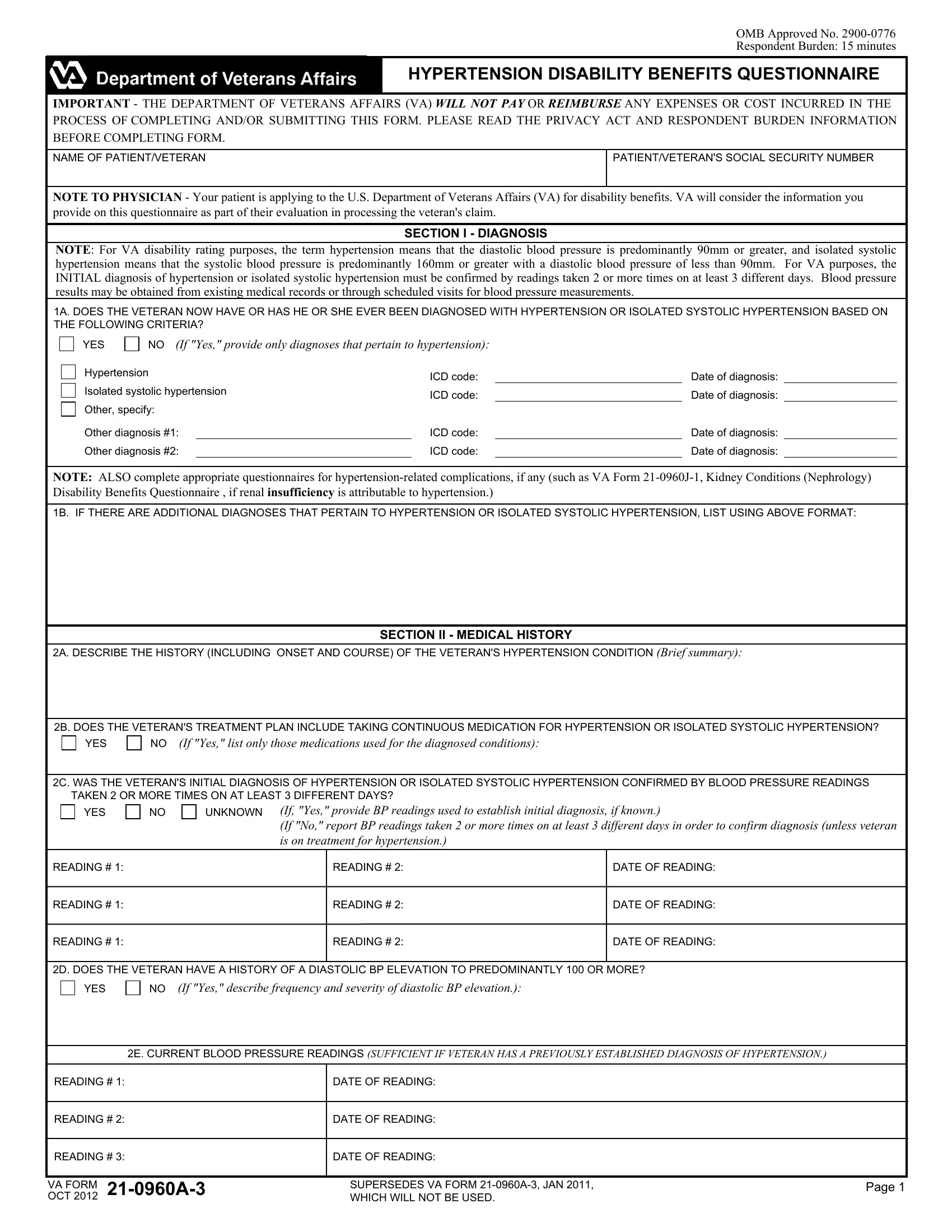
1. The 2012 requires specific details to be inserted. Make sure the subsequent fields are complete:
2. Right after completing the previous part, head on to the next stage and enter the essential details in these blank fields - A DESCRIBE THE HISTORY INCLUDING, B DOES THE VETERANS TREATMENT PLAN, YES, If Yes list only those medications, C WAS THE VETERANS INITIAL, YES, UNKNOWN, If Yes provide BP readings used to, READING, READING, DATE OF READING, READING, READING, READING, and READING.
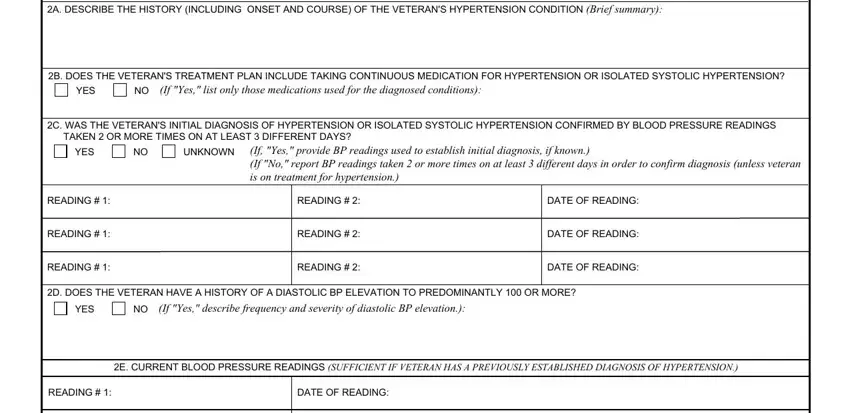
3. This third step is easy - complete all the fields in READING, READING, DATE OF READING, DATE OF READING, VA FORM OCT, SUPERSEDES VA FORM A JAN WHICH, and Page to finish this segment.

4. Filling out A DOES THE VETERAN HAVE ANY SCARS, YES, NO If Yes complete Item B, B ARE ANY OF THE SCARS PAINFUL, YES, NO If Yes ALSO complete VA Form F, C DOES THE VETERAN HAVE ANY OTHER, YES, NO If Yes describebrief summary, DOES THE VETERANS HYPERTENSION OR, YES, NO If Yes describe the impact of, and SECTION IV FUNCTIONAL IMPACT is paramount in the next section - make sure you invest some time and take a close look at every single blank area!
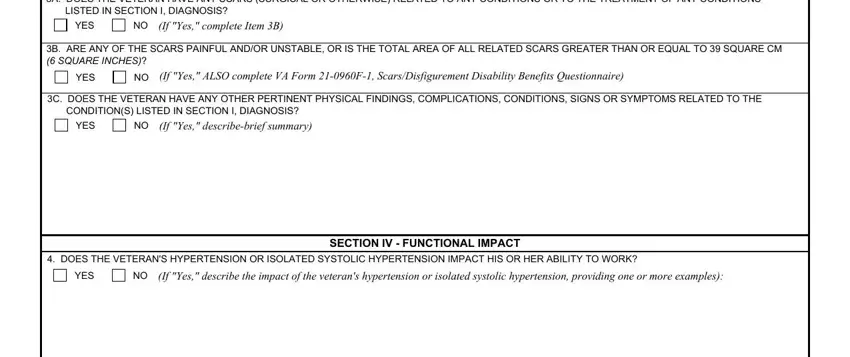
People who use this PDF generally make errors when completing NO If Yes describebrief summary in this part. Make sure you reread what you enter here.
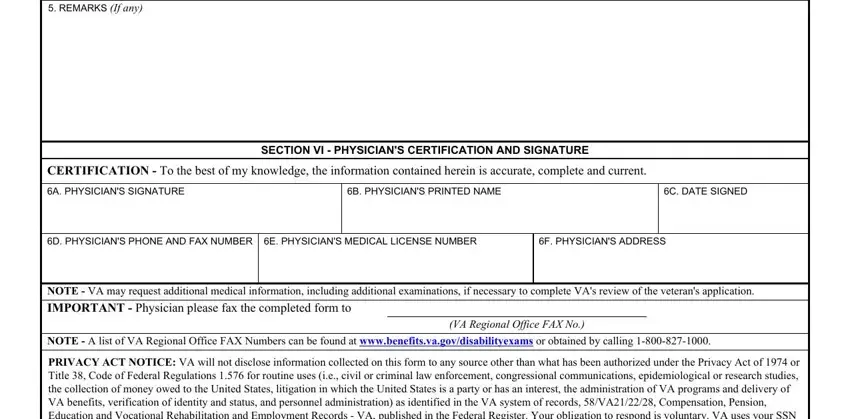
5. The pdf must be completed by going through this segment. Here you can find a full list of blank fields that require correct information for your form usage to be faultless: REMARKS If any, CERTIFICATION To the best of my, A PHYSICIANS SIGNATURE, B PHYSICIANS PRINTED NAME, C DATE SIGNED, SECTION VI PHYSICIANS, D PHYSICIANS PHONE AND FAX NUMBER, E PHYSICIANS MEDICAL LICENSE NUMBER, F PHYSICIANS ADDRESS, NOTE VA may request additional, IMPORTANT Physician please fax, NOTE A list of VA Regional Office, VA Regional Office FAX No, and PRIVACY ACT NOTICE VA will not.
Step 3: Before obtaining the next stage, double-check that all blanks were filled out as intended. Once you’re satisfied with it, click on “Done." Get hold of your 2012 once you subscribe to a 7-day free trial. Instantly access the pdf in your FormsPal cabinet, with any modifications and adjustments being automatically synced! Here at FormsPal, we do our utmost to make sure that all your details are kept private.