
Should you desire to fill out va form 21 22a printable, it's not necessary to download any kind of software - simply use our PDF editor. Our expert team is always endeavoring to enhance the tool and help it become much better for users with its multiple functions. Enjoy an ever-improving experience today! This is what you'll have to do to get going:
Step 1: Click on the "Get Form" button in the top area of this page to access our PDF tool.
Step 2: As soon as you launch the online editor, you will notice the document prepared to be filled in. Besides filling in different blank fields, you might also perform other things with the form, such as putting on custom words, editing the initial text, inserting images, affixing your signature to the PDF, and much more.
In an effort to complete this document, ensure you type in the necessary details in every blank:
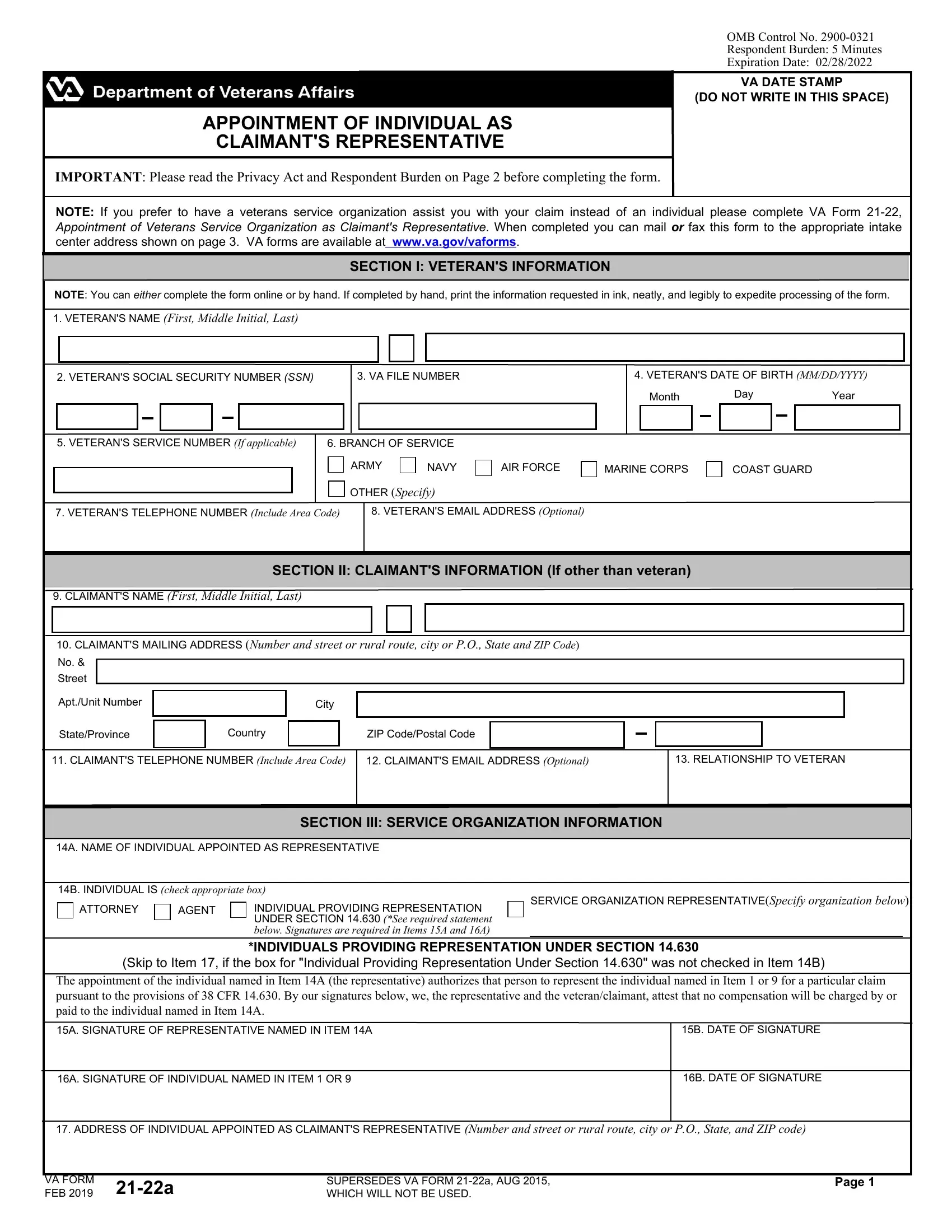
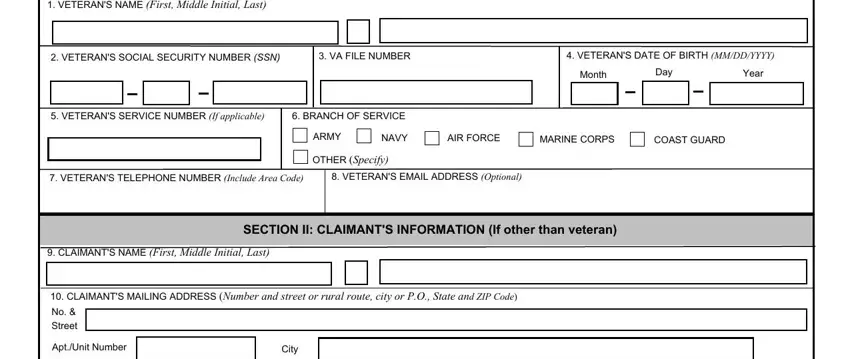
1. The va form 21 22a printable requires specific details to be entered. Make sure the subsequent blank fields are finalized:
2. Once your current task is complete, take the next step – fill out all of these fields - StateProvince, Country, ZIP CodePostal Code, CLAIMANTS TELEPHONE NUMBER, CLAIMANTS EMAIL ADDRESS Optional, RELATIONSHIP TO VETERAN, SECTION III SERVICE ORGANIZATION, A NAME OF INDIVIDUAL APPOINTED AS, B INDIVIDUAL IS check appropriate, ATTORNEY, AGENT, INDIVIDUAL PROVIDING, SERVICE ORGANIZATION, Skip to Item if the box for, and The appointment of the individual with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
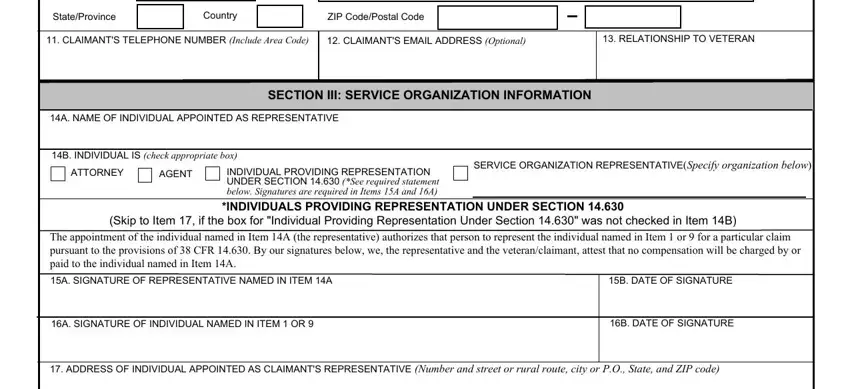
People often make errors while filling in SECTION III SERVICE ORGANIZATION in this part. You need to read again what you enter right here.
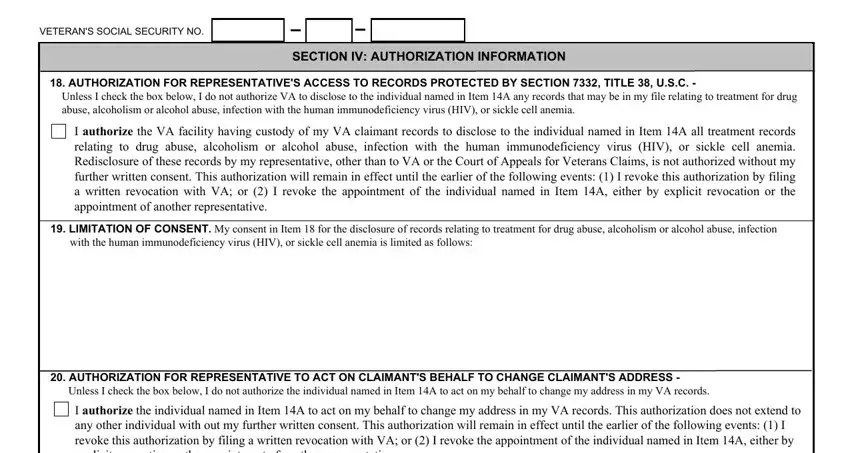
3. The following step is rather easy, VETERANS SOCIAL SECURITY NO, SECTION IV AUTHORIZATION, AUTHORIZATION FOR REPRESENTATIVES, Unless I check the box below I do, I authorize the VA facility having, LIMITATION OF CONSENT My consent, AUTHORIZATION FOR REPRESENTATIVE, Unless I check the box below I do, and I authorize the individual named - all these fields is required to be filled in here.
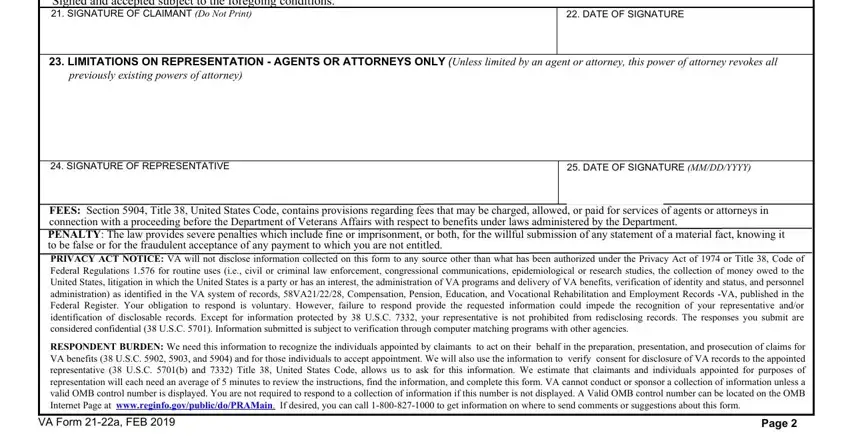
4. Filling out I the person named in Item or, DATE OF SIGNATURE, LIMITATIONS ON REPRESENTATION, previously existing powers of, SIGNATURE OF REPRESENTATIVE, DATE OF SIGNATURE MMDDYYYY, FEES Section Title United States, RESPONDENT BURDEN We need this, VA Form a FEB, and Page is crucial in this fourth step - be sure to spend some time and be mindful with every single field!
Step 3: After you've reviewed the information in the blanks, click "Done" to complete your form at FormsPal. After getting a7-day free trial account at FormsPal, you'll be able to download va form 21 22a printable or email it right off. The document will also be readily accessible via your personal account page with your each edit. With FormsPal, you can complete forms without worrying about personal information leaks or records getting distributed. Our protected system ensures that your personal information is kept safe.