
va form 21 22 printable can be filled in very easily. Simply use FormsPal PDF editing tool to get it done in a timely fashion. Our tool is continually developing to grant the best user experience attainable, and that is thanks to our dedication to constant enhancement and listening closely to user feedback. It just takes several basic steps:
Step 1: Click the orange "Get Form" button above. It's going to open up our pdf editor so that you could start completing your form.
Step 2: When you access the online editor, you will notice the document prepared to be filled out. Besides filling in various fields, you may as well do several other actions with the form, including writing custom textual content, modifying the initial text, inserting illustrations or photos, placing your signature to the form, and much more.
It is simple to fill out the pdf following our helpful tutorial! This is what you should do:
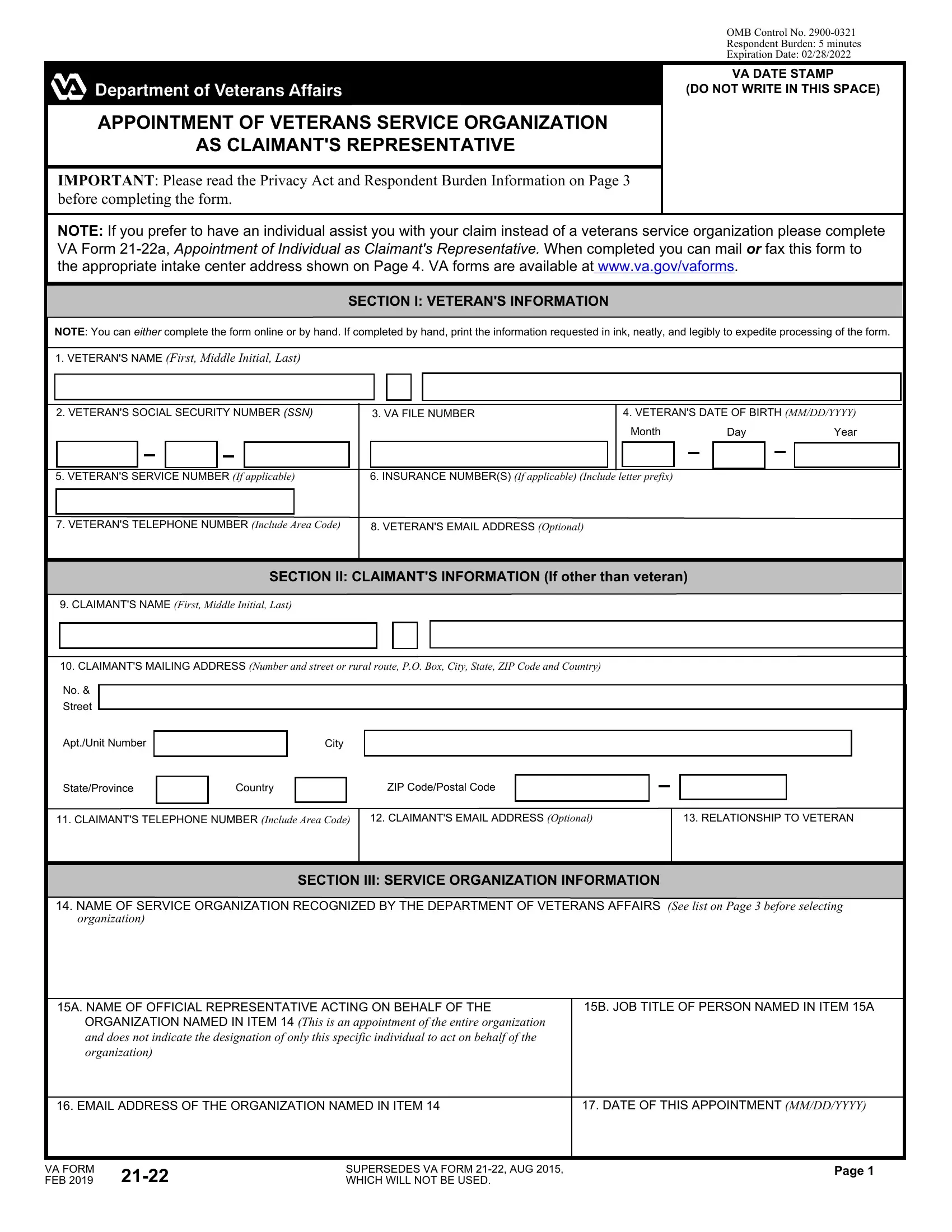
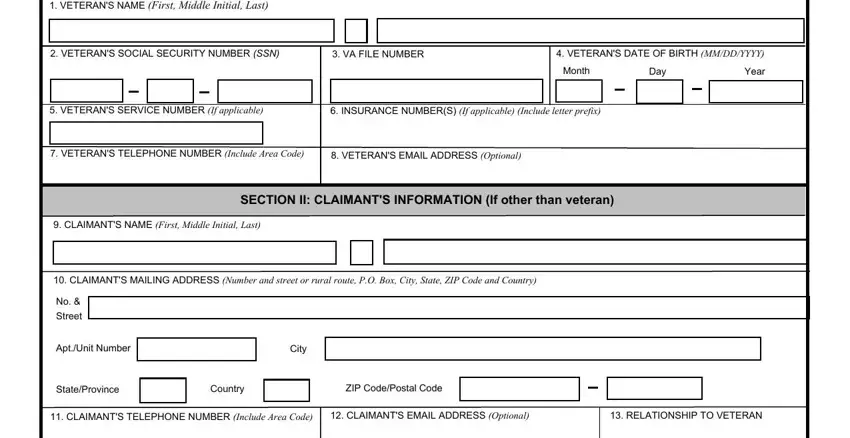
1. Fill out your va form 21 22 printable with a group of major blanks. Consider all the necessary information and ensure absolutely nothing is neglected!
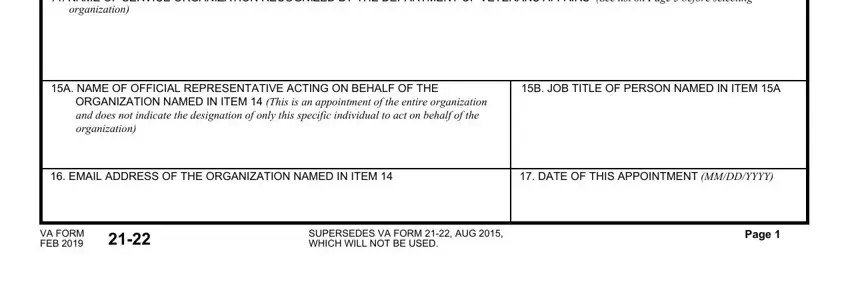
2. Once your current task is complete, take the next step – fill out all of these fields - NAME OF SERVICE ORGANIZATION, A NAME OF OFFICIAL REPRESENTATIVE, B JOB TITLE OF PERSON NAMED IN, EMAIL ADDRESS OF THE ORGANIZATION, DATE OF THIS APPOINTMENT MMDDYYYY, VA FORM FEB, SUPERSEDES VA FORM AUG WHICH, and Page with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. The next part is normally simple - fill out all of the blanks in VETERANS SOCIAL SECURITY NUMBER, SECTION IV AUTHORIZATION, AUTHORIZATION FOR REPRESENTATIVES, I authorize the VA facility having, LIMITATION OF CONSENT I authorize, DRUG ABUSE, INFECTION WITH THE HUMAN, ALCOHOLISM OR ALCOHOL ABUSE, SICKLE CELL ANEMIA, AUTHORIZATION TO CHANGE CLAIMANTS, and I authorize any official to complete the current step.
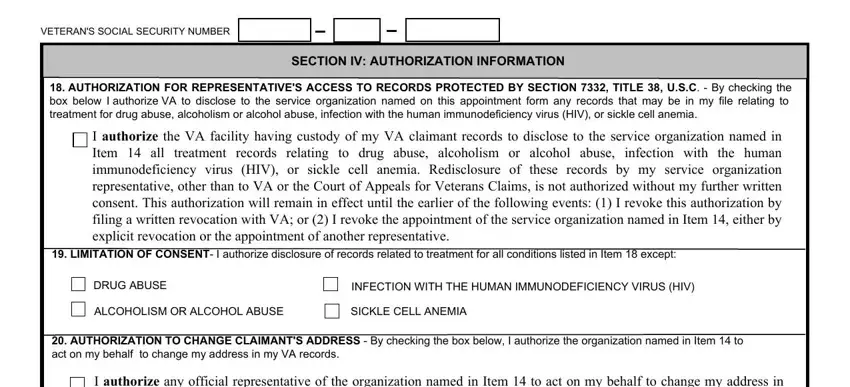
You can potentially get it wrong while filling out the LIMITATION OF CONSENT I authorize, hence ensure that you go through it again before you'll send it in.
4. It's time to complete this next segment! In this case you'll get these A SIGNATURE OF VETERAN OR CLAIMANT, B DATE SIGNED, A SIGNATURE OF VETERANS SERVICE, B DATE SIGNED, NOTE As long as this appointment, COPY OF VA FORM SENT TO, DATE SENT, ACKNOWLEDGED Date, REVOKED Reason and date, VRE FILE, EDU FILE, VA USE, ONLY, LG FILE, and INSURANCE FILE empty form fields to fill out.
Step 3: Ensure that your information is accurate and simply click "Done" to finish the process. Right after registering a7-day free trial account with us, it will be possible to download va form 21 22 printable or send it through email immediately. The form will also be accessible through your personal account menu with all your edits. We don't sell or share any information that you enter while completing forms at FormsPal.