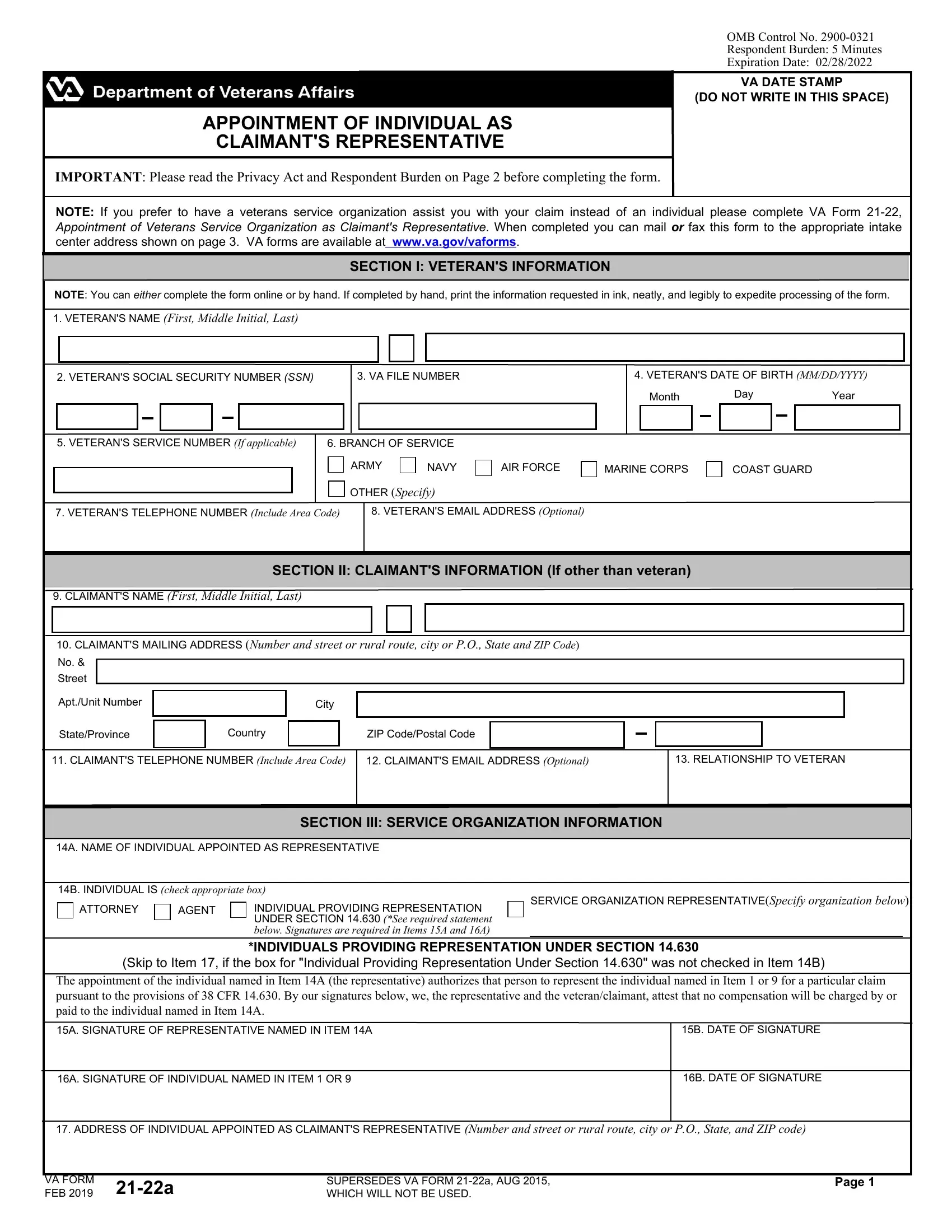
The VA Form 21-22a plays a critical role in the veterans' benefits claims process, functioning as the official document for appointing an individual as a veteran's representative. This form is integral for veterans who opt for personal representation in navigating the often complex proceedings of claiming benefits from the Department of Veterans Affairs (VA). By completing this form, a veteran can authorize an individual - whether an attorney, an agent, or a person providing representation under certain sections of the Code of Federal Regulations - to act on their behalf. This appointed representative is thereby empowered to prepare, present, and prosecute claims to the VA, ensuring the veteran's interests are adequately represented. Furthermore, the form outlines the conditions under which the representative can access the veteran's records, including sensitive health information, with provisions for limiting such access. It also includes a section where the veteran can specify the extent of authorization for the representative to act on their behalf, such as changing the veteran's address on VA records. The inclusion of checks and balances, such as the prohibition of fees without proper authorization, along with severe penalties for fraudulent claims, underscores the form's importance in safeguarding the integrity of the representation process. The VA Form 21-22a not only facilitates veteran representation but also exemplifies the structured approach towards ensuring veterans' rights and access to benefits are protected and efficiently advanced.
| Question | Answer |
|---|---|
| Form Name | Va Form 21 22A |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | va form 21 22 pdf, va form 21 22a fillable, 21 22a, va form 21 22a instructions |