
You are able to complete form va 21 4140 without difficulty in our online editor for PDFs. To have our tool on the forefront of efficiency, we work to integrate user-oriented capabilities and improvements on a regular basis. We are at all times glad to receive feedback - join us in revolutionizing the way you work with PDF docs. To get the process started, take these basic steps:
Step 1: Access the PDF in our editor by clicking the "Get Form Button" above on this webpage.
Step 2: Once you launch the editor, you will notice the form prepared to be filled out. Other than filling out various blank fields, it's also possible to perform some other things with the file, such as putting on your own textual content, changing the original text, inserting graphics, signing the document, and more.
Be attentive while filling in this pdf. Ensure all necessary fields are completed correctly.
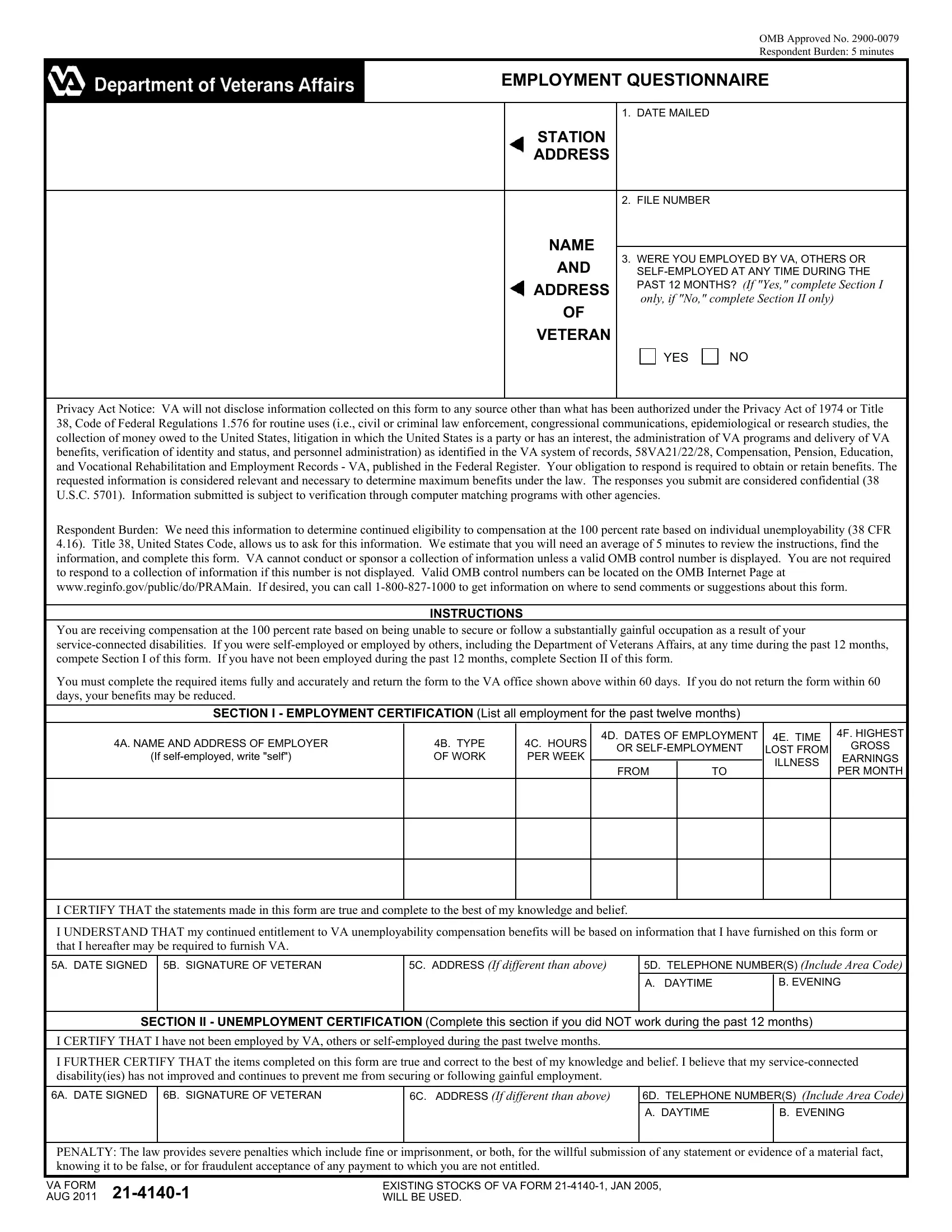
1. To get started, once completing the form va 21 4140, start with the section containing next blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - If selfemployed write self, B TYPE OF WORK, C HOURS PER WEEK, FROM, ILLNESS, EARNINGS PER MONTH, I CERTIFY THAT the statements made, I UNDERSTAND THAT my continued, A DATE SIGNED B SIGNATURE OF, C ADDRESS If different than above, D TELEPHONE NUMBERS Include Area, A DAYTIME, B EVENING, SECTION II UNEMPLOYMENT, and I CERTIFY THAT I have not been with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
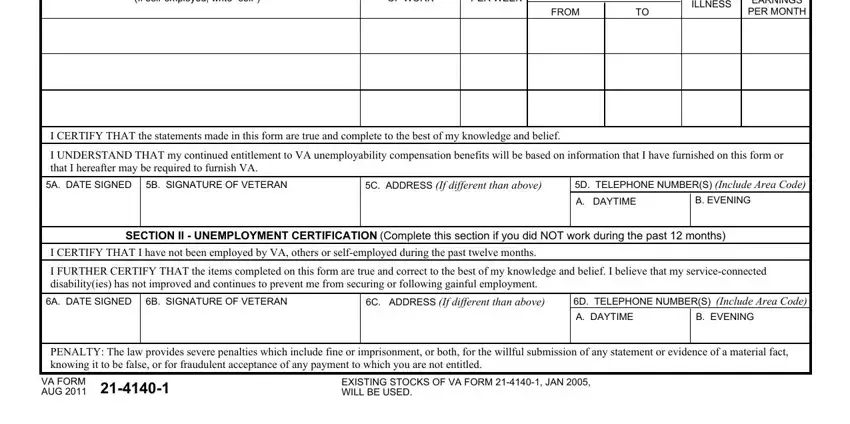
A lot of people often make some mistakes when completing I UNDERSTAND THAT my continued in this area. You need to review everything you type in right here.
Step 3: Right after going through the filled in blanks, click "Done" and you're good to go! Get hold of the form va 21 4140 once you join for a 7-day free trial. Quickly get access to the pdf form inside your personal cabinet, with any modifications and adjustments all kept! We don't sell or share the details that you use while working with forms at FormsPal.