The PDF editor you will begin using was developed by our top level web programmers. You can easily complete the va form 21 526b pdf document promptly and effortlessly using this application. Just stick to this guideline to start out.
Step 1: First of all, click the orange "Get form now" button.
Step 2: After you've entered the va form 21 526b pdf edit page, you'll see all actions it is possible to take concerning your file within the top menu.
Provide the data required by the application to get the document.
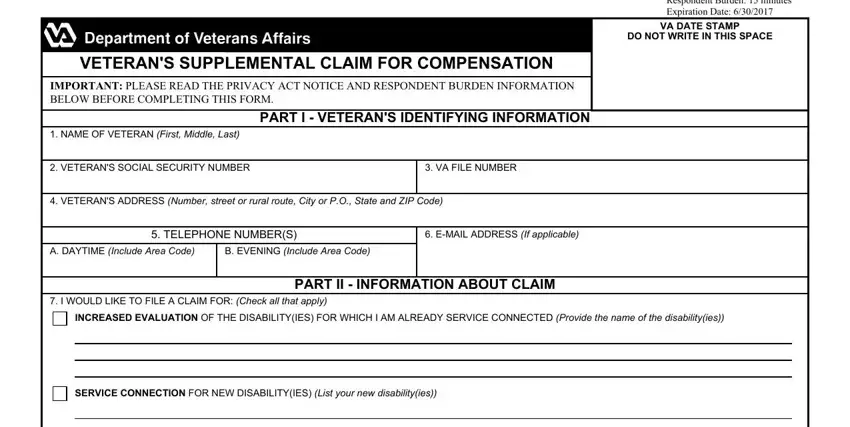
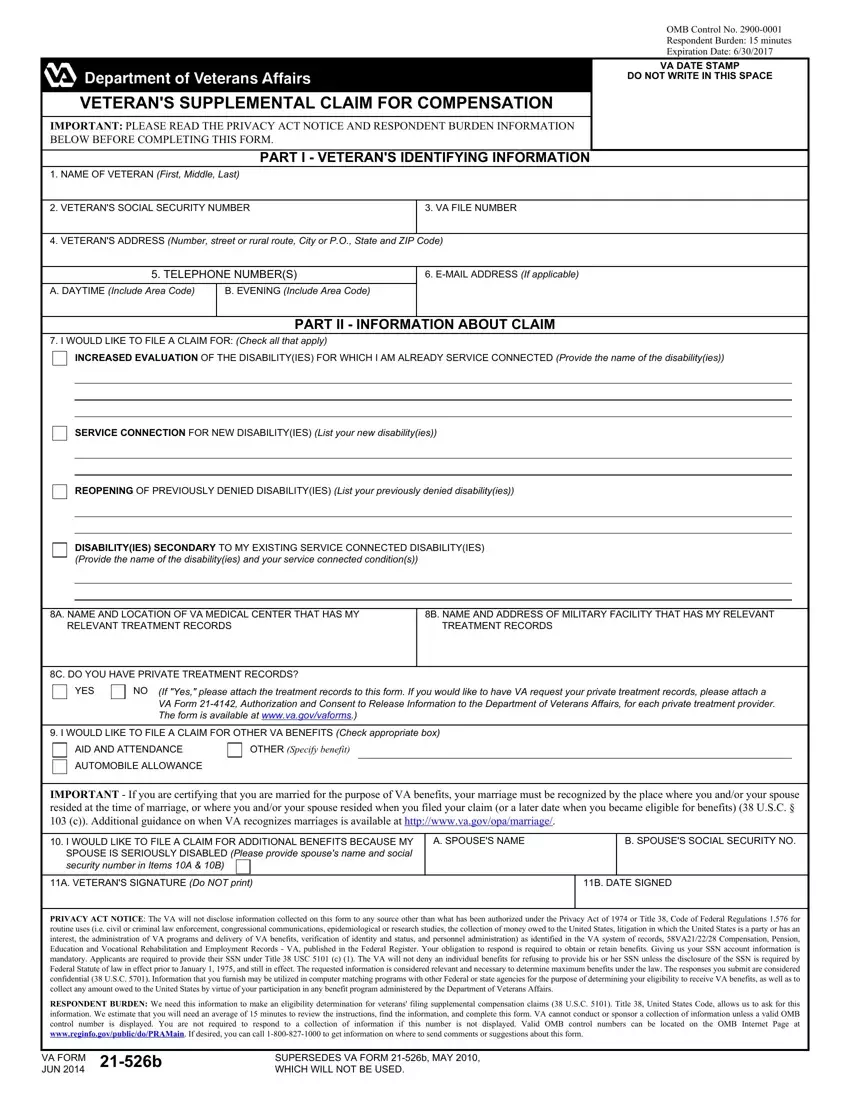
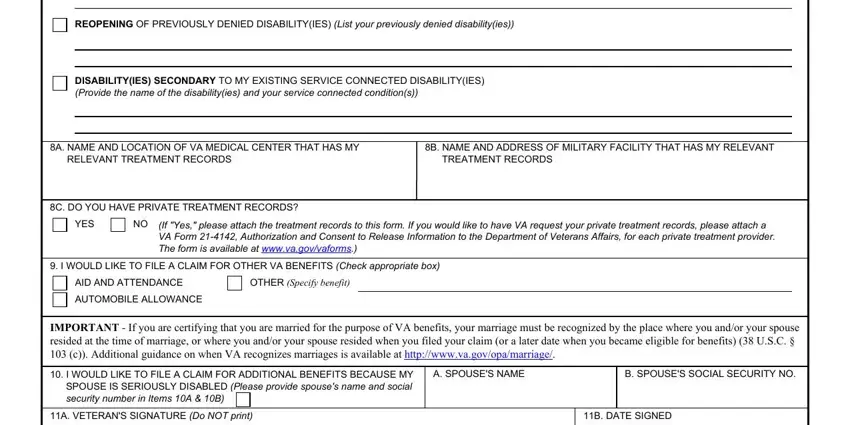
You have to type in your data in the section REOPENING OF PREVIOUSLY DENIED, DISABILITYIES SECONDARY TO MY, A NAME AND LOCATION OF VA MEDICAL, B NAME AND ADDRESS OF MILITARY, RELEVANT TREATMENT RECORDS, TREATMENT RECORDS, C DO YOU HAVE PRIVATE TREATMENT, YES, If Yes please attach the treatment, I WOULD LIKE TO FILE A CLAIM FOR, AID AND ATTENDANCE, OTHER Specify benefit, AUTOMOBILE ALLOWANCE, IMPORTANT If you are certifying, and I WOULD LIKE TO FILE A CLAIM FOR.
Step 3: Click the "Done" button. Next, you can transfer your PDF document - download it to your device or deliver it via email.
Step 4: Create a duplicate of each form. It's going to save you time and enable you to avoid challenges down the road. By the way, your data will not be distributed or analyzed by us.
