
When working in the online tool for PDF editing by FormsPal, you're able to fill out or edit va bdd form here and now. To have our tool on the forefront of convenience, we aim to adopt user-driven capabilities and enhancements on a regular basis. We are routinely looking for feedback - help us with remolding PDF editing. With a few basic steps, you can begin your PDF journey:
Step 1: Firstly, access the tool by clicking the "Get Form Button" at the top of this page.
Step 2: As soon as you start the editor, you'll notice the form ready to be filled in. Apart from filling in various blanks, you may as well do other things with the Document, that is adding your own words, changing the initial text, inserting images, placing your signature to the document, and more.
This PDF will need particular info to be typed in, hence you should take the time to type in what's expected:
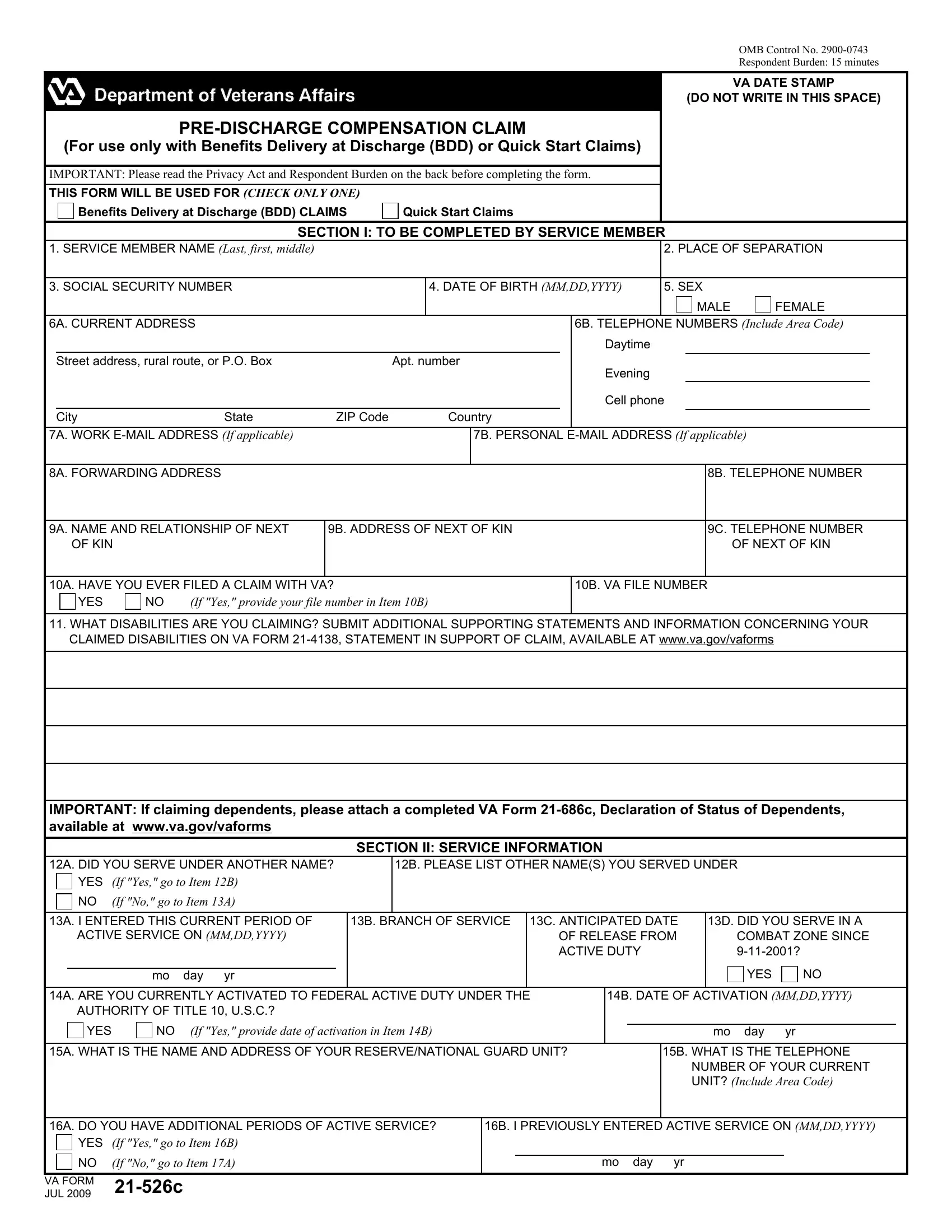
1. It is very important complete the va bdd form accurately, thus pay close attention when filling in the segments including all of these blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - IMPORTANT If claiming dependents, A DID YOU SERVE UNDER ANOTHER NAME, B PLEASE LIST OTHER NAMES YOU, SECTION II SERVICE INFORMATION, YES, If Yes go to Item B, If No go to Item A, A I ENTERED THIS CURRENT PERIOD OF, B BRANCH OF SERVICE, ACTIVE SERVICE ON MMDDYYYY, C ANTICIPATED DATE OF RELEASE FROM, D DID YOU SERVE IN A, COMBAT ZONE SINCE, mo day yr, and YES with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This subsequent part is normally quite uncomplicated, A WHAT IS THE NAME AND ADDRESS OF, B WHAT IS THE TELEPHONE, NUMBER OF YOUR CURRENT UNIT, A DO YOU HAVE ADDITIONAL PERIODS, B I PREVIOUSLY ENTERED ACTIVE, YES, If Yes go to Item B, NO If No go to Item A, VA FORM, JUL c, and mo day yr - all these empty fields will have to be filled in here.

4. This next section requires some additional information. Ensure you complete all the necessary fields - A WILL YOU RECEIVE RETIRED PAY, YES, If Yes complete Item B, B TYPE OF RETIRED PAY, LONGEVITY, DISABILITY, TDRL, SECTION III MILITARY RETIRED PAY, A WILL YOU RECEIVE ANY TYPE OF, B LIST AMOUNT If known, C LIST TYPE If known, YES, If Yes complete Items B and C, IMPORTANT Unless you check the box, and If you receive both military - to proceed further in your process!
5. This document should be finalized by going through this part. Further there can be found an extensive listing of fields that require accurate details for your document submission to be accomplished: the bank where you want your, at the bottom left of your check, SECTION V CERTIFICATIONS AND, I certify and authorize the, B DATE SIGNED, A SIGNATURE OF WITNESS If claimant, B PRINTED NAME AND ADDRESS OF, SECTION VI WITNESSES TO SIGNATURE, A SIGNATURE OF WITNESS If claimant, B PRINTED NAME AND ADDRESS OF, and PRIVACY ACT NOTICE The form will.
Regarding SECTION VI WITNESSES TO SIGNATURE and at the bottom left of your check, be certain you get them right in this current part. Those two are surely the key fields in this form.
Step 3: After you've glanced through the information in the file's blanks, click "Done" to complete your FormsPal process. Get the va bdd form when you join for a 7-day free trial. Readily use the pdf within your personal account page, together with any modifications and adjustments being automatically preserved! When you work with FormsPal, you can fill out forms without having to worry about information leaks or records getting distributed. Our protected platform makes sure that your personal information is maintained safely.