VA FORM
JUN 2014
1.
private medical treatment records for the child's pertinent disabilities
3. Report for any VA medical examinations VA determines are necessary to decide your claim.
If claiming benefits for a seriously disabled (helpless) child of the veteran, all, if any, relevant,
VA Form 21-674, Request for Approval of School Attendance
. veteran, a copy of the birth certificate or court record of adoption showing relation to the veteran If claiming benefits for a child of the veteran between the ages of 18 and 23, a completed
.
Housebound Status or Permanent Need for Regular Aid and Attendance, and a completed VA Form 21-0779, Request for Nursing Home Information in Connection with Claim for Aid and Attendance
Requirements for Certain Claimants:
Under. the circumstances shown below, you must also submit simultaneously with your claim:
If claiming benefits as the surviving spouse of the veteran, a copy of your marriage certificate showing your marriage to the veteran, or if claiming benefits for a child or biological/adoptive parent of the
If claiming DIC with increased survivor benefits, a completed VA Form 21-2680, Examination for
Stood in Relation of Parent
benefits as the foster parent of the veteran, a completed VA Form 21-524, Statement of Person Claiming to Have
If claiming DIC as the parent of the veteran, all necessary income and net-worth information and, if claiming
All, if any, relevant, private medical treatment records and an identification of any relevant treatment records
If claiming DIC:
.
.available at a Federal facility, such as a VA medical center, that support your claim
.Any and all Service Treatment and Personnel Records in the custody of the veteran's Guard or Reserve Unit(s)
.
2. Submit simultaneously with your claim:
A copy of the veteran's Death Certificate (unless he or she died on active duty); AND
If claiming death pension:
.. All necessary income and net-worth information
If claiming death pension with increased survivor benefits, a completed VA Form 21-2680, Examination for Housebound Status or Permanent Need for Regular Aid and Attendance, and a completed VA Form 21-0779, Request for Nursing Home Information in Connection with Claim for Aid and Attendance
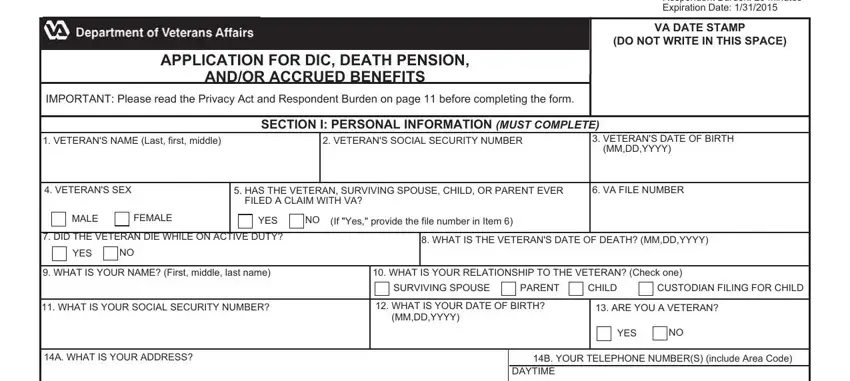
Submit your claim on a signed and completed VA Form 21-534EZ, Application for DIC, Death Pension, and/or Accrued Benefits (Attached).
NOTICE TO SURVIVOR OF EVIDENCE NECESSARY TO SUBSTANTIATE A CLAIM FOR
DEPENDENCY AND INDEMNITY COMPENSATION, DEATH PENSION, AND/OR
ACCRUED BENEFITS
(This notice is applicable to survivors claims for: Death Pension • Dependency Indemnity Compensation (DIC) • DIC under 38 U.S.C. 1151 • Increased Survivor Benefits Based on Need for Aid and Attendance or Being Housebound • Accrued Benefits • Benefits Based on a Veteran's Seriously Disabled Child)
Use this notice and the attached application to submit a claim for DIC, Death Pension, and/or Accrued Benefits.
This notice informs you of the evidence necessary to substantiate your claim.
Want your claim processed faster? The Fully Developed Claim (FDC) Program is the fastest way to get your claim processed, and there is no risk to participate! To participate in the FDC Program if you are making a claim for DIC, Death Pension, and/or Accrued Benefits, simply submit your claim in accordance with the "FDC Criteria" shown below. If you are making a claim for veterans disability compensation or related compensation benefits, use VA Form 21-526EZ, Application for Disability Compensation and Related Compensation Benefits. If you are making a claim for veterans non service-connected pension benefits, use VA Form 21-527EZ, Application for Pension. VA forms are available at www.va.gov/vaforms.
FDC Criteria (Claim(s) for DIC, Death Pension, and/or Accrued Benefits)
21-534EZ |
SUPERSEDES VA FORM 21-534EZ, DEC 2012, |
Page 1 |
|
WHICH WILL NOT BE USED. |
|
|
|
The Fully Developed Claim (FDC) Program is the fastest way to get your claim processed, and there is no risk to participate!
Participation in the FDC Program is optional and will not affect the quality of care you receive or the benefits to which you are entitled. If you file a claim in the FDC Program and it is determined that other records exist and VA needs the records to decide your claim, then VA will simply remove the claim from the FDC Program (Optional Expedited Process) and process it in the Standard Claim Process. See below for more information. If you wish to file your claim in the FDC Program, see FDC Program (Optional Expedited Process). If you wish to file your claim under the process in which VA traditionally processes claims, see Standard Claim Process.
WHAT YOU NEED TO DO
You must submit all relevant evidence in your possession and provide VA information sufficient to enable it to obtain all relevant evidence not in your possession. If your claim involves a disability the veteran had before entering service and that was made worse by service, please provide any information or evidence in your possession regarding the health condition that existed before the veteran's entry into service.
FDC Program (Optional Expedited Process)
You must:
•Submit your claim in accordance with the "FDC Criteria" (see page 1)
Standard Claim Process
You must:
•If you know of evidence not in your possession and want VA to try to get it for you, give VA enough information about the evidence so that we can request it from the person or agency that has it
If the holder of the evidence declines to give it to VA, asks for a fee to provide it, or otherwise cannot get the evidence, VA will notify you and provide you with an opportunity to submit the information or evidence. It is your responsibility to make sure we receive all requested records that are not in the possession of a Federal department or agency.
HOW VA WILL HELP YOU OBTAIN EVIDENCE FOR YOUR CLAIM
FDC Program (Optional Expedited Process)
VA will:
•Retrieve relevant records from a Federal facility, such as a VA medical center, that you adequately identify and authorize VA to obtain
Standard Claim Process
VA will:
•Retrieve relevant records from a Federal facility that you adequately identify and authorize VA to obtain
•Make every reasonable effort to obtain relevant
records not held by a Federal facility that you adequately identify and authorize VA to obtain. These may include records from state or local governments and privately held evidence and information you tell us about, such as private doctor or hospital records or records from current or former employers
WHEN YOU SHOULD SEND WHAT WE NEED
FDC Program (Optional Expedited Process) |
Standard Claim Process |
You must:
•Send the information and evidence simultaneously with your claim
If you submit additional information or evidence after you submit your "fully developed" claim, then VA will remove the claim from the FDC Program expedited process and process it in the Standard Claim process. If we decide your claim before one year from the date we receive the claim, you will still have the remainder of the one-year period to submit additional information or evidence necessary to support the claim.
We strongly encourage you to:
• Send any information or evidence as soon as you can
You have up to one year from the date we receive the claim to submit the information and evidence necessary to support your claim. If we decide the claim before one year from the date we receive the claim, you will still have the remainder of the one year period to submit additional information or evidence necessary to support the claim.
WHERE TO SEND INFORMATION AND EVIDENCE
Mail or take your application and any evidence in support of your claim to the closest VA regional office. VA regional office addresses are available on the Internet at www.va.gov/directory.
VA FORM 21-534EZ, JUN 2014 |
Page 2 |
WHAT THE EVIDENCE MUST SHOW TO SUPPORT YOUR CLAIM
|
If you are claiming... |
See the evidence table titled... |
|
Needs-based benefits based on the veterans wartime service. |
Death Pension |
|
|
|
|
• The veteran's death was related to his or her service (DIC), OR |
|
|
• DIC benefits because the veteran was receiving or entitled to |
Dependency and Indemnity Compensation (DIC) |
|
|
|
receive benefits for a service-connected disability rated totally |
|
|
disabling. |
|
|
The veteran's death was a result of VA medical treatment, |
DIC under 38 U.S.C. 1151 |
|
vocational rehabilitation, or compensated work therapy. |
|
|
|
DIC and it was previously denied by VA. |
Reopened DIC |
|
Increased death pension or DIC benefits because your disabilities |
Increased Survivor Benefits Based on Need for Aid and |
|
cause you to be in need of aid and attendance or to be confined |
Attendance or Being Housebound |
|
to your residence. |
|
|
|
|
|
|
You are eligible to the benefits that were due to the veteran at |
Accrued Benefits |
|
the time of the veteran's death. |
|
|
|
You are eligible to the benefits because a child of the veteran is |
Helpless Child |
|
severely disabled. |
|
|
|
EVIDENCE TABLES |
|
Death Pension
To support your claim for death pension benefits, the evidence must show:
1.The veteran met certain minimum requirements regarding active service during a period of war. Generally, those requirements involve:
•90 days of consecutive service, at least one day of which was during a period of war; OR
•90 days of combined service during at least one period of war;
(Note : If the veteran's service began after September 7, 1980, additional length-of-service requirements may apply, typically requiring two years of continuous service or completion of active-duty obligations.)
OR any length of active service during a period of war when:
•At the time of death, the veteran was receiving (or entitled to receive) VA disability compensation or retirement pay for a service-connected disability; OR
•The veteran was discharged from active service due to a service-connected disability.
2.Your net worth and income do not exceed certain requirements.
Dependency and Indemnity Compensation (DIC)
To support a claim for Dependency and Indemnity Compensation (DIC) benefits based on a service-connected disability established during the veteran's lifetime, the evidence must show:
•The veteran died while on active service; OR
•The veteran had a service-connected disability(ies) that was either the principal or contributory cause of the veteran's death; OR
•The veteran died from non service-connected injury or disease AND was receiving, or entitled to receive VA compensation for a service-connected disability rated totally disabling:
•For at least 10 years immediately before death; OR
•For at least 5 years after the veteran's release from active duty preceding death; OR
•For at least 1 year before death, if the veteran was a former prisoner of war who died after September 30, 1999
To support a claim for DIC benefits based on a disability that was not service-connected or for which the veteran did not file a claim during his or her lifetime, the evidence must show:
•An injury or disease that was incurred or aggravated during active service, or an event in service that caused an injury or disease; AND
•A physical or mental disability that was either the principle or contributory cause of death. This may be shown by
medical evidence or by lay evidence of persistent and recurrent symptoms of disability that were visible or observable; AND
•A relationship between the disability associated with the cause of death and an injury, disease, or event in service. This may be shown by medical records or medical opinion or, in certain cases, by lay evidence
VA FORM 21-534EZ, JUN 2014 |
Page 3 |
EVIDENCE TABLES (Continued)
Dependency and Indemnity Compensation (DIC) (Continued)
To support your claim for DIC benefits based upon the service person's active duty for training, the evidence must show:
•The service person was disabled during active duty for training due to a disease or injury incurred in the line of duty, and the disease or injury caused or contributed to the service person's death.
If VA granted service connection for a disease or injury during the service person's lifetime, evidence that the service-connected disease or injury caused or contributed to the service person's death may satisfy this requirement.
To support a claim for DIC benefits based on a disability that was not service-connected or for which the service person did not file a claim during his or her lifetime, the evidence must show:
•The service person was disabled during active duty for training due to a disease or injury incurred in the line of duty; AND
•A physical or mental disability that was either the principle or contributory cause of death. This may be shown by medical evidence or by lay evidence of persistent and recurrent symptoms of disability that were visible or observable; AND
•A relationship between the principal or contributory cause of death and the disability due to injury or disease, incurred in the line of duty. This may be shown by medical records or medical opinions or, in certain cases, by lay evidence.
To support your claim for DIC benefits based upon the service person's inactive duty training, the evidence must show:
•The service person died during inactive duty training due to an injury incurred or aggravated in the line of duty, or acute myocardial infarction, cardiac arrest, or cerebrovascular accident during such training; OR
•The service person was disabled during inactive duty training due to an injury incurred or aggravated in the line of duty, or acute myocardial infarction, cardiac arrest, or cerebrovascular accident that occurred during such training; and that injury, acute myocardial infarction, cardiac arrest, or cerebrovascular accident caused or contributed to the service person's death
If VA granted service connection for an injury, acute myocardial infarction, or cerebrovascular accident during the service person's lifetime, evidence that the service-connected condition caused or contributed to the service person's death may satisfy this requirement.
To support a claim for DIC benefits based on a disability that was not service-connected or for which the service person did not file a claim during his or her lifetime, the evidence must show:
•The service person was disabled during inactive duty training due to an injury incurred or aggravated in the line of duty, or acute myocardial infarction, cardiac arrest, or cerebrovascular accident that occurred during such training; AND
•The injury, acute myocardial infarction, cardiac arrest, or cerebrovascular accident caused or contributed to the service person's death
DIC under 38 U.S.C. 1151:
In order to support your claim for DIC under 38 U.S.C. 1151, the evidence must show:
•The deceased veteran died as a result of undergoing VA hospitalization, medical or surgical treatment, examination, or training; AND
•The death was:
•the direct result of VA fault such as carelessness, negligence, lack of proper skill, or error in judgment; OR
•the direct result of an event that was not a reasonably expected result or complication of the VA care or treatment; OR
•the direct result of participation in a VA Vocational Rehabilitation and Employment or compensated work therapy program
Reopened DIC:
In order to reopen a claim previously denied by VA, we need new and material evidence. New and material evidence must raise a reasonable possibility of substantiating your claim. The evidence cannot simply be repetitive or cumulative of the evidence we had when we previously decided your claim. VA will make reasonable efforts to help you obtain currently existing evidence.
However, we cannot provide a medical examination or obtain a medical opinion until your claim is successfully reopened.
•To qualify as new, the evidence must currently exist and be submitted to VA for the first time
•In order to be considered material, the additional existing evidence must pertain to the reason your claim was previously denied
VA FORM 21-534EZ, JUN 2014 |
Page 4 |
EVIDENCE TABLES (Continued)
Increased Survivor Benefits Based on Need for Aid and Attendance or Being Housebound
In order to support your claim for increased survivor benefits based on the need for aid and attendance, the evidence must show:
•you have corrected vision of 5/200 or less in both eyes; OR
•you have concentric contraction of the visual field to 5 degrees; OR
•you are a patient in a nursing home due to mental or physical incapacity; OR
•you require the aid of another person in order to perform personal functions required in everyday living, such as bathing, feeding, dressing yourself, attending to the wants of nature, adjusting prosthetic devices, or protecting yourself from the hazards of your daily environment (38 Code of Federal Regulation 3.352(a)); OR
•you are bedridden, in that your disability or disabilities requires that you remain in bed apart from any prescribed course of convalescence or treatment (38 Code of Federal Regulation 3.352(a)); OR
In order to support your claim for increased benefits based on being housebound, the evidence must show:
• you are substantially confined to your immediate premises because of permanent disability
Accrued Benefits:
To support a claim for accrued benefits, the evidence must show:
•Benefits were due the veteran based on existing ratings, decisions, or evidence in VA's possession at the time of death, but the benefits were not paid before the veteran's death; AND
•You are the surviving spouse, child, or dependent parent of the deceased veteran
VA pays accrued benefits in the following order of priority:
1.Spouse
2.Children of the veteran (in equal shares)
3.Dependent parents (in equal shares)
Helpless Child:
To support a claim for benefits based on a veteran's child being helpless, the evidence must show that the child, before his or her 18th birthday, became permanently incapable of self-support due to a mental or physical disability.
IMPORTANT
If you are certifying that you are married for the purpose of VA benefits, your marriage must be recognized by the place where you and/or your spouse resided at the time of marriage, or where you and/or your spouse resided when you filed your claim (or a later date when you became eligible for benefits) (38 U.S.C. § 103(c)). Additional guidance on when VA recognizes marriages is available at http://www.va.gov/opa/marriage/.
HOW VA DETERMINES THE EFFECTIVE DATE
If we grant a claim for death benefits, the beginning date of your entitlement will generally be based on when we received your claim However, if VA received your claim within one year of the date of the veteran's death, entitlement will be from the first day of the month in which the veteran died.
The veteran's death certificate is evidence relevant to determining the effective date of any benefits we award.
Higher levels of benefits are available for a veteran's surviving spouse and/or parents who are unable to perform certain activities of daily living or leave their home. Higher levels of benefits may be effective from the date medical evidence first establishes entitlement.
For more information on the FDC Program, visit our web site at http://benefits.va.gov/transformation/fastclaims/ For more
information on VA benefits, visit our web site at www.va.gov, contact us at http://iris.va.gov, or call us toll-free at 1-800-827-1000. If you use a Telecommunications Device for the Deaf (TDD), the number is 1-800-829-4833.
VA forms are available at www.va.gov/vaforms.
VA FORM 21-534EZ, JUN 2014 |
Page 5 |